 whiteflame (PRO)
whiteflame (PRO)Thanks to Larz for joining this debate, as I'm sure this will be a fantastic one for his presence participation! I'm looking forward to it.
I'll start with some housekeeping:
The topic is a little broad, allowing me to choose what vaccines I would define as “some.” I could defend multiple vaccines as important, but that would make my case rather complex and increase my burdens unnecessarily. As such, I will be advocating solely for the MMR vaccine.
So what is the MMR vaccine? The acronym stands for measles, mumps and rubella, three single-stranded RNA viruses, and the vaccine is meant to impart a protective immunologic response to those who take it. The vaccine is composed of live attenuated viruses, meaning that their virulence has been strongly reduced, but the virus is still viable. This ensures that the vaccine will have the strongest and longest-lasting effect, meaning that the vaccine only has to be taken in its two-shot series once over a person's lifetime.
But that only defines the two terms – some and vaccinations. What does it mean to be mandatory? I will define that contextually by providing a model.
The U.S. Federal Government will require that all individuals before attending school receive the vaccination, which applies for home schooling by age 5. All individuals who are beyond schooling age and under the age of 65 would have to get the vaccine within 5 years. These will be subsidized on an as-needed basis, ensuring that it is broadly affordable. Failure to vaccinate oneself or one's family results in a fine that scales with income. There would be other exclusions based on allergies, pregnancies, and those individuals who are immunocompromised.
With that, I'll into some contentions.
1. Disease Spread
We must recognize that vaccination is not a choice that solely affects the individual being vaccinated. The decision to get the MMR vaccine affects everyone around you. Measles, mumps and rubella are all transmitted through droplets that are sprayed into the air, making them airborne pathogens with a high likelihood of transmission to those around the infected.[1, 2, 3] The mere fact that others are put at risk by people who refuse to take these vaccines creates a substantial societal harm in the status quo, as many are allowed to refuse to get the vaccine.
We're living this harm today, seeing a resurgence in these entirely preventable diseases in the U.S. and abroad.[4] This resurgence is most marked with measles, a disease that the U.S. had eliminated by the year 2000, but which returned in 17 outbreaks among 222 people just in 2011.[5] Mumps has had 4 reported outbreaks this year alone, and has had several small and two large outbreaks in the last 5 years, encompassing thousands of people.[6] Rubella has also returned from a long absence, appearing in three cases in the U.S. in 2012 after being eliminated back in 2004.[7] This change resulted mainly from a false public perception that vaccines have been linked to autism.[8]
In order to understand why vaccinating a large portion of the population is necessary, we have to understand the term “herd immunity.” This has been defined differently by different authors, but I will use the term in this fashion: “a particular threshold proportion of immune individuals that should lead to a decline in the incidence of infection.”[9] What that means is that if someone becomes sick with a given disease, herd immunity would ensure that that person is so much more likely to run into someone vaccinated against that disease than someone who is vulnerable that they would be extremely unlikely to infect other people. We cannot possibly vaccinate everyone and achieve absolute immunity because of the necessity of the exclusions I listed in my case, but we can seek to achieve herd immunity.
What does that threshold look like for these diseases? For measles, this is 95%.[10] For mumps, it's at least 88%, though it “may need to be higher” than this previously established threshold.[11] For rubella, it sits at 90%.[12] Only through mandatory vaccination could we ever hope to reach those numbers.
2. Disease Impact
My first contention established a threshold for harm in status quo, but I will now show that that threshold has a tremendous impact on society. In order to understand that, we have to know what the impact of these three diseases is.
Measles:
“Prior to the vaccine, 3-4 million people were infected in the U.S. each year, resulting in 48,000 hospitalizations, 400-500 deaths and approximately 1,000 who developed chronic disabilities.
Even with modern medical care, the disease can lead to serious complications, including blindness, pneumonia, otitis media and severe diarrhea. Despite the availability of a vaccine it remains a leading cause of death among young children worldwide, with deaths mainly attributable to the complications of the disease...
More than 90 percent of susceptible people, usually unvaccinated, develop the disease after being exposed. There is no treatment except to make the patient as comfortable as possible by keeping them hydrated and trying to control the fever. Unvaccinated young children and pregnant women are at the highest risk for measles and its complications, including death.”[13]
Mumps:
“Mumps is not normally a fatal disease, and up to 30% of mumps infections are asymptomatic. There can be serious complications, however, including aseptic meningitis, orchitis, oophoritis, mastitis, pancreatitis, and deafness. Meningitis occurs in up to 10% of mumps cases; it is usually subclinical and self-limiting. Symptoms of mumps-related meningitis include fever, headache, vomiting, and neck stiffness, which peak for a period of 48 hours before resolution and might appear up to 1 week before parotid swelling. More serious neurologic symptoms are rare and are due to encephalitis. Hearing loss following mumps infections is rare (1 in 2000 to 30,000 cases) and usually results in mild to moderate hearing loss.
Orchitis [swelling of the testicles] occurs 4 to 8 days after the onset of parotitis and is a common complication, affecting 20% of men who develop mumps after puberty. Of those cases, 40% will develop testicular atrophy and 30% will have lasting changes in sperm count, sperm motility, and sperm morphology.”[14]
Rubella:
While the disease usually only results in a light fever and small rash, this disease is mainly problematic for pregnant women. “In 1964-65, America had a major rubella epidemic, with more than 12 million cases and 20,000 babies born with congenital rubella; of these, 13,000 were deaf, 3,500 were blinded by congenital cataracts, and 1,800 more suffered severe cognitive impairment.”[7] Since pregnant mothers are among the few who cannot get the vaccine, every single person who decides not to get the vaccine is putting these mothers at risk.
Taken together, this means these three viruses present as enduring, broad threats to public health that are made dramatically worse in the absence of herd immunity.
I now leave it to Lars to present his case/rebut mine.
1. http://www.cdc.gov/measles/about/transmission.html
2. http://www.cdc.gov/mumps/about/transmission.html
3. http://www.cdc.gov/rubella/about/index.htm
5. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6115a1.htm
6. http://www.cdc.gov/mumps/outbreaks.html
8. http://online.wsj.com/news/articles/SB10001424127887323300004578555453881252798
9. http://cid.oxfordjournals.org/content/52/7/911.full
10. http://www.theguardian.com/society/2013/apr/25/measles-mmr-the-essential-guide
11. http://jid.oxfordjournals.org/content/202/5/655.full
12. http://www.ncbi.nlm.nih.gov/pubmed/23099870
13. http://guardianlv.com/2014/07/measles-resurgence-in-u-s-after-development-of-vaccine-in-1966/
14. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3135444/
Return To Top | Posted:
 admin (CON)
admin (CON)Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services...
In America!

Return To Top | Posted:
admin: You quote plenty of figures of how things were prior to vaccination. Can you explain to me the relevance of these figures to the debate?whiteflame: They tell a story regarding the likelihood of certain complications. I'm establishing a numerical link between incidence of disease and incidence of each complication.whiteflame: Where did you get the "scientific advice" that Coca-Cola and comfort are cures for mumps and rubella, respectively?admin: avoid acidic drinks for mumps: http://www.northgatepractice.co.uk/Library/Conditions/Articles/mumps/treatment , just wait around for rubella to pass: http://www.northgatepractice.co.uk/Library/Conditions/Articles/rubella/treatmentadmin: Would you say that complication rates are the same today as they were prior to vaccination? If not, would you say vaccination was primarily responsible for the change?whiteflame: Just a note: neither of those "treatments" are cures, as Lars initially professed them to be. They ameliorate the symptoms, they do not affect the ability of the virus to replicate or interact with any given cell type.admin: Wait - I said they're not cures. I said they're advice by scientists for people who have the disease. In the next sentence I say there are no cures.admin: Now stop arguing in the CX and answer my questionwhiteflame: You did use the word "cure," but fine, I'll move on.whiteflame: I'd say the complication rates are higher. We've both agreed that they happen mainly among those who are immunocompromised, and as, even today, each of these individuals represents a larger subset of the population without vaccinations, they are more likely to be infected in any given outbreak. I'd say that vaccination has altered the rate of complications among the infected by shifting the population that's able to become infected.admin: Not sure I get the logic but let me clarify this first: if I was to check, as a proportion of all infected, the death rate for MMR in the last ten years, you're telling me it will be higher than it was a century ago in the USA?whiteflame: No. My claim is that a higher proportion of the infected population today would experience complications. A great deal more of the population today is immunized, so no, the epidemics wouldn't be as large. But each epidemic is more likely to include immunocompromised individuals than it was previously, as a result of their inability to be vaccinated. If it's going to spread, it's more likely today to spread to someone who is immunocompromised.admin: Other than to substitute "complications" for "death rate", is there any material difference between that and what I said? If not, do you not see the death rate as a complication?whiteflame: I realized after I wrote it that I didn't read the question correctly. My answer would be a qualified yes. I see death as a complication, but one we can better control for today than we could 10 years ago.admin: OK cool. So the first half of this year the USA has seen almost 300 measles cases and no deaths or serious brain complications (http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htm). Is this just a freak statistical accident to you?whiteflame: It's 300 people. If you look at the numbers I provided in my first round, 300 cases isn't enough to see serious complications. You're still talking about a relatively small population. I wouldn't characterize it as a "freak accident," but rather as lacking in statistical significance.whiteflame: Do you consider the possible side effects that someone suffers as a result of mandatory vaccination a loss to their rights?admin: Yes.admin: In your rounds, you cite a death rate for measles above 1% immediately before vaccination. So I'd assume from that you'd expect more than 3 to have died this year. How do you explain the lack of measles deaths at all in the US for some many years now?whiteflame: Three is a very small number and not statistically distant enough from 0 to be measured and evaluated as changing how we should view measles infections in the U.S. We're talking about data gathered among millions of infections and trying to make conclusions based on 300 is unreasonable.admin: Do you know when the last time is somebody died of measles in the USA?whiteflame: I have it at 2005, though I think it's unreasonable to assess the impact of measles on the U.S. solely on the basis of recent deaths, especially when the number of infections is on a substantial uptick.admin: I have it at 2003 but that's fine. So roughly a decade of no deaths. Would you say that whenever the rate of measles rises in the general population, the death rate from measles should then also rise?whiteflame: Two things. One, I already mentioned that our ability to respond to complications and prevent deaths has improved substantially over the past 10 years, so no, I don't suspect it would rise. That doesn't mean that those complications don't occur, they're just tackled early and strongly in most cases. Two, I also already mentioned that the numbers we're dealing with are still relatively small. We're not dealing in numbers sufficient for statistical significance to be evaluated.admin: OK, look at this graph. Notice the LARGE sample size and HISTORIC data from prior to a decade to. Prior to vaccination, would it be fair to say measles rates were rising while deaths were falling?  whiteflame: Do you consider the spread of a disease through negligence to other people to be a loss of rights?admin: Nowhiteflame: ...Lars, I understand where you're going with this, and I've already given you my response multiple times - changes to medical care affect the number of deaths that occur. Antibiotics became much more widely used during that same time period. It's no surprise that the bacterial infections that so often accompany these viral infections started being less of a problem when patients are being treated for the bacterial infection. Death rates fell prior to vaccination, but complications were the same.whiteflame: What makes the second circumstance substantially different from the first?admin: Mandatory vaccination is different from mandatory infection in that the infected couldn't help it. Both have a loss of power, but only in the former do you give up your rights to somebody else.admin: So what complications would you say are a significant enough threat today from MMR that will affect everybody?admin: (*sorry, probably should have said "could affect" and not "will affect")
whiteflame: Do you consider the spread of a disease through negligence to other people to be a loss of rights?admin: Nowhiteflame: ...Lars, I understand where you're going with this, and I've already given you my response multiple times - changes to medical care affect the number of deaths that occur. Antibiotics became much more widely used during that same time period. It's no surprise that the bacterial infections that so often accompany these viral infections started being less of a problem when patients are being treated for the bacterial infection. Death rates fell prior to vaccination, but complications were the same.whiteflame: What makes the second circumstance substantially different from the first?admin: Mandatory vaccination is different from mandatory infection in that the infected couldn't help it. Both have a loss of power, but only in the former do you give up your rights to somebody else.admin: So what complications would you say are a significant enough threat today from MMR that will affect everybody?admin: (*sorry, probably should have said "could affect" and not "will affect") whiteflame: I'd say most complicating infections are problematic enough to be significant. Pneumonia would top my list. I would also have a problem with permanent disease states incurred like hepatitis. The major blood diseases would as well, though less so.whiteflame: So the only loss of rights that matters is one in which rights are lost to someone else? On that basis, who are you losing rights to when you get a side effect from vaccination?admin: You are losing rights whenever the vaccination is mandatory. The side effects are irrelevant to the question. There you're losing rights to the government. Rights analysis is about obligations people hold towards one another. To say viruses have human rights is absurd.admin: Looking at pneumonia. If I get measles, what's the chance I will develop pneumonia?whiteflame: Based on the CDC's numbers, 1 in 20 children get pneumonia, though I can't find specific numbers for adults. http://www.cdc.gov/measles/about/complications.html This year, between January and May, there have been 5, which represents slightly less than that. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htmwhiteflame: I guess I didn't get as clear of an answer to this as I'd thought earlier. You now say that the side effects are irrelevant to the question. Are you now saying that those side effects that result from mandatory vaccination are not abrogations of the rights of those individuals who acquire them?admin: Any effects resulting from mandatory vaccinations are abrogations of rights. Even if the vaccine were 100% effective and had no side effects, making it mandatory would abrogate people's rights.admin: Do you agree with the WHO that the best way to avoid getting pneumonia is through nutrition, environmental factors, and getting a flu jab?whiteflame: I would agree that those are beneficial, but insufficient. Measles specifically makes a person more vulnerable to pneumonia. That's actually the same purpose of the "flu jab," which is meant to prevent you from getting influenza, another major virus associated with pneumonia infections. Nutrition and environmental factors can certainly have an effect, but merely changing circumstances for the better is insufficient. It's also not possible for everyone to change those factors.whiteflame: Alright, I'm still confused by your answer. I understand that your view is that people's rights are harmed by mandatory vaccination independent of side effects. What you seem to be saying is that the side effects are a further abrogation of rights. But you said earlier that surrendering rights was the concern. Who are those rights surrendered to?admin: Side effects are not a further abrogation of rights. If somebody chooses between two medications, they do not inherently limit their human rights by choosing one that may have side effects.admin: I guess my point though, is, isn't pneumonia also rather easily treated and prevented, compared to other illnesses?whiteflame: Not always. Pneumonia can be caused by a wide variety of bacterial diseases, many of which require different treatments and not all of which are easily distinguished. There's also the reality that antibiotic resistance is becoming more and more of a problem, and specifically pneumococcal pneumonia has presented with a great deal of concerns in this regard. http://www.cdc.gov/pneumococcal/drug-resistance.htmlwhiteflame: I feel like I'm not getting a consistent answer here. You said "any effects resulting from mandatory vaccinations are abrogations of rights." Now you're saying that side effects are not a further abrogation of rights. Is there something unique to side effects that ensures that they do not represent a loss of rights? Or are you saying that only in the instance where the vaccine is mandated is there a further abrogation of rights that results from side effects?admin: They're not further abrogations of rights, but part of the same abrogation. The vaccine and all its effects abrogate your rights because of the mandate.admin: OK, I'll save most of my analysis on this for my round. Moving on. Why do you think there's a measles outbreak in the US this year?whiteflame: I'd say the likeliest explanation is two-fold %u2013 one, there's a major outbreak in the Philippines, which is spreading to this country, and two, there's a reduced level of vaccination across the U.S. population. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htmwhiteflame: Alright, I think that answer is straightforward, so I'll go with that. Next question: is approaching herd immunity beneficial, even if we don't achieve it?admin: Noadmin: What makes you believe the level of vaccination in the US is reduced?whiteflame: The CDC's data indicates as much. http://deadstate.org/new-cdc-report-thanks-to-anti-vaccine-hysteria-u-s-measles-cases-have-tripled-in-2013/ Individual state analysis has at least been done for Texas. healthblog.dallasnews.com/2014/08/vaccination-rates-for-kids-are-down-rates-of-infectious-diseases-are-up.html/whiteflame: So increased of immunity are not beneficial if they don't reach herd immunity levels?admin: Yesadmin: (can you repost your link? leads to a page not found page for me)admin: (sorry, my fault)admin: OK - just read both of them. What I don't understand is - are those sources not aware that there's been a consistent upward trend in MMRII vaccine uptake since 2003?whiteflame: I'd like to see your source for that.whiteflame: So you contend that a larger portion of the population taking the MMR vaccine isn't beneficial if that population doesn't cause the country to herd immunity?whiteflame: to reach* herd immunityadmin: Yesadmin: Will provide my sources in round. What proportion of people do you think would be the ideal proportion to have immunized?whiteflame: I've already given idealized numbers on the basis of what is required for herd immunity. I recognize that those aren't currently achievable.admin: So roughly 95%?whiteflame: Optimally, yes.whiteflame: So what is the purpose of immunization, then, from your perspective? Does having sub-herd immunity levels of vaccination harm a population, or do you view it as a net 0? And please, explain this perspective with more than a few words.admin: I think it depends on the vaccination. Different vaccinations have different risks and benefits that different people have to individually evaluate; its purpose just like any other medicine. In my own personal evaluation, I don't consider the MMR vaccine to be a good enough medicine to justify its cost.admin: If I were to provide a credible source, in round, showing that the current MMR vaccination rate is roughly 94.5% for all kindergarten-age kids, would you give up?whiteflame: As that is still sub-optimum and we should be attempting to reach that optimum in any case, that point would not force me to surrender. If anything, that would provide proof that it's possible to reach that threshold of 95%, unless you could show that my policy wouldn't increase the number of vaccinated individuals.whiteflame: Alright, but that means you're factoring other aspects into your answer. Imagine that there were no side effects, and that people were choosing to get the vaccine instead of being required to get it. Would you say that there's a benefit to a more substantial portion of the population receiving that optimized MMR vaccine?admin: In terms of public health, there's a benefit. The same kind of argument could be made for eugenics if you factor no other aspects into your answer.admin: So that 0.5% would be enough to convince you that you need to introduce a mandatory program for everybody?whiteflame: Yes. It would tell me that 94.5% of the population would be practically unaffected by the mandate and receive benefits from the subsidies, while the remaining 5.5% would be affected, bringing the country to the level of herd immunity in the process.whiteflame: Alright, that's enough for that line of questioning. Was mandating vaccination for smallpox a net harm?admin: I don't think so. It was an early experiment and a lot went wrong, but ultimately in my personal view the good outweighed the harm. I would defend the right of others to see that differently if they wanted.admin: Do you believe it was OK for Hitler to force-medicate Jews, gypsys etc?whiteflame: No.whiteflame: What makes mandatory medication for smallpox a net benefit?admin: I didn't read your question right, sorry. If it was mandatory it would be a net harm. What makes it a net harm is that it's mandatory. If you're just looking at the vaccine itself, I'd say it was a net benefit because although the vaccine had its problems it cured a really bad threat.admin: Why is it OK for you to force-medicate but not Hitler?whiteflame: ...If you really want a list of reasons, we can go there. 1) I'm not force medicating. I'm not strapping anyone down and making them take a shot in the arm. 2) Hitler didn't force medicate solely under the auspices of public health. 3) The basis for his force-medication was pseudoscience. 4) I'm not singling out racial groups. This list could go on and on, but I'll stop there.whiteflame: Would you contend that smallpox would no longer be a problem today if no one had ever mandated vaccination for it?admin: No. Smallpox was eradicated in numerous countries with no mandates.admin: In your answer, I note that you DON'T say the Nuremberg principle of consent. Do you believe that Hitler violated any medical ethics by failing to obtain consent?whiteflame: Hitler violated multiple codes of ethics, and yes, I'd say that his choice to force people to be medicated entirely against their will without recourse and therefore completely without any level of consent is problematic. I would also say that those moral failings don't appear in my case.whiteflame: I'm noticing that's not really an answer to my question. Would smallpox have been eradicated from the world as a whole if there had never been any mandates that people take the vaccine?admin: Yes. The vaccine wasn't the only reason it went away, and although it definitely helped, the mandates were not required to ensure high uptake.admin: Is it true that your model imposes a cost on people for doing nothing?whiteflame: It imposes a cost on people who negligently put others at risk, so no, I wouldn't say it's for doing nothing.whiteflame: By what means, and please be specific, would smallpox have been eradicated worldwide in the absence of vaccination?whiteflame: (sorry for the double posts... don't know why that happened...)admin: I never said it would, but that the vaccine was not the only reason. It could not have been done without the vaccine, but better nutrition, better public health, improvements to sanitation and a better understanding of the disease all contributed. Would be happy to expand on all that in my round.admin: Does an unvaccinated person really inherently put other people at risk, or is that only if they actually catch the disease?whiteflame: I'd argue that in the case of these diseases, unvaccinated persons cannot reasonably assume that they will never be exposed to at least one these diseases in their lifetimes. These are airborne viruses with a simple route of transmission that anyone but the most isolated persons risks acquiring.admin: Can a government reasonably assume a person will never jaywalk in their lifetime?whiteflame: No. That's why states have laws against it.whiteflame: (I'll get back to asking more questions later. Right now, I'm just interested in seeing where you're going with this)admin: They have laws against it when you do it, they do not presume in advance that you will and punish you for that. Is my understanding of the law accurate?whiteflame: If you would like to argue that the better alternative is to punish people for getting and spreading these diseases, I will be happy to address that, though I'd like you to flesh out how you would apply a similar method to an infectious disease. I don't think the transition is straightforward and that it creates more problems than it solves.admin: I take it then that it's accurate. Are there not laws in force already restricting the rights of people with diseases like measles, such as rules preventing them from going to school?whiteflame: I don't recall any such laws being pervasive in the U.S., nor are they binding for all schools. Such laws would also be ineffective at preventing the spread of disease, only cutting off one route of transmission. I'd say they're incapable of solving for the problem, and their presence only masks the problem.admin: Do you agree that immunization has a 1-10% failure rate? And further, do you agree that staying away from the disease has a 0% failure rate?whiteflame: Yes, though I would say that the failure rate trends towards the lower end. And yes, if you could tell me a way to completely avoid any chance of transmission of these diseases, "staying away from" them would be more effective, if exceedingly unlikely.whiteflame: You mentioned botched production systems for vaccines. How commonly do incidents occur in the U.S. where vaccinations are manufactured poorly, leading to illness/injury?admin: Nowadays, extremely rarely. The chance has been reduced significantly over the past century. As I established in my case, however, the smallness of the chance is actually irrelevant.admin: If somebody has a compromised immune system, would they not avoid people who have measles etc (literally) like the plague?whiteflame: You seem to be making a few basic assumptions here. One, that someone who has the measles is going to present with symptoms that are obvious while they are infectious. Two, that those symptoms are obviously separate from other common illnesses. Three, that they can avoid all individuals who might be sick without placing themselves in a large plastic bubble. And four, that even if they take intense precautions, that they can avoid indirect infections. It is not simple even if one is taking the fewest risks possible.whiteflame: I read the Murphy's Law contention. Why should voters prefer huge impacts that are extremely unlikely to substantial and still likely impacts?admin: Judges should be free to make up their own mind as to whether potential risks outweigh potential benefits for any medication. I'm simply showing science-supported valid justifications also exist for not taking the vaccine. Many will not accept that argument, and that's fine. I wish them well. It's not me in this debate who is trying to force my opinion on other people.admin: What other "common illness" looks like measles or mumps symptoms-wise that an immune-compromised person would NOT want to avoid like the plague?whiteflame: We've been through the symptoms, I don't think I need to repeat them. Yes, an immunocompromised person would want to avoid them as well. But there are two problems. One, this dramatically increases the number of people that those who are immunocompromised have to avoid, making the process all the more impossible. Two, we're talking about basic symptoms like "fever," "dry cough" and "sore throat," which are simulated quite well by several non-disease states. These aren't necessarily hallmarks of disease, and so aren't so simple to recognize as signs of someone to stay away from.whiteflame: Nice jab. Still, could you tell me the most recent date when a poorly manufactured vaccine led to illness/injury in the U.S.?admin: No because the VICP does not usually make rulings as to what exactly was wrong with the vaccine, only whether the vaccine was at fault at all. Usually there's no real way of telling. It's safe to say that it's rare.admin: What's more likely today - that an immune-compromised person will die from a shark attack or that they will die from measles, mumps or rubella?whiteflame: I won't speculate, though if they're immunocompromised, the process of leaving their home, heading to the beach, getting settled and entering the water all present as opportunities to be infected by those around them. It seems rather unlikely that an immunocompromised individual would further compromise themselves by swimming out far enough to put themselves at risk.admin: If they're not willing to go out to sea, assuming that's true, then can we agree that they'll definitely try to not go near people showing symptoms of those illnesses?whiteflame: We can assume what they'll try to do. We cannot assume that they would be capable of achieving it without encasing themselves in plastic.whiteflame: You mentioned that deaths that occur as a result of measles tend to come from complicating infections. How do most die from influenza and the human immunodeficiency virus?admin: They ALWAYS come from complicating infections. Even in immune-compromised persons - the virus itself is extraordinarily benign. The mechanism for death is similar to influenza or HIV when it occurs in that there are complicating infections, but the virus is far less deadly than either.admin: Do you agree that among the 0.3% killed by complications related to measles among infected in the decade before last, there were only (roughly) 0.045% were immune deficient? Do you further agree that in the last decade, 0% of immune deficient persons who have contracted measles have died?whiteflame: I'm not going to agree to numbers without seeing the sources themselves and validating their findings, so while that may be accurate, I would need to see the support behind them.whiteflame: Is it your contention, then, that the complicating factors that accompany these virus infections are not enhanced significantly (especially in immunosuppressed persons) by the viral infections themselves?admin: Not significantly. The enhancement is minor at best.admin: Since you're making the claim that the harm is particularly strong to immunosuppressed people, do you have any statistics that support that claim in relation to MMR specifically from the past two decades or so?whiteflame: I'll be all too happy to provide primary and secondary evidence in the next round that shows that measles, in particular, presents a tremendous risk to the immunosuppressed, and further that it can and does induce immunosuppression. admin: But are these sources statistics from the past two decades relating to MMR in immunosuppressed people specifically?whiteflame: Would you also say that measles does not have a significant immunosuppressive effect?admin: Yeswhiteflame: Would you say that influenza has a higher immunosuppressive effect? And, if so, what differentiates the two?whiteflame: Yes. If these studies did occur before 20 years ago, though, the effects remain the same. We may be better able to address the resulting fallout today, but that immunosuppression still occurs because we have limited or no understanding of the mechanisms involved.admin: Yes, but not much. Their respective RNA and how that causes them to behave is what differentiates them for the most part, as with pretty much any RNA viruses. I kind of don't understand the point of the question.admin: You say the effects are the same as 20 years ago. Does this mean you believe that the environment plays no difference in how the disease affects people, or are you saying the environment is the same today as 20 years ago?whiteflame: "Environment" is a pretty broad term and can encompass a number of very different variables. Of course there's differences in the environment. Whether those differences are substantial enough to dramatically affect disease progression for the majority of the population that gets measles is another story. If it's your view that there's a substantial environmental difference between the 1990's and the 2010's that is likely to do this, then you should make that difference clear.whiteflame: I'm pretty well versed on viral RNAs myself, so I'll go with what you've given me on that front. Has vaccine-derived illness ever been characterized in people receiving the MMR vaccine? Similarly, has there ever been an instance of transmission of a separate disease to patients receiving the MMR vaccine?admin: Yes, quite frequently. A small outbreak of measles from the vaccine, for example, is observed in about 5% of people who get the MMR vaccine. One of the side effects is literally getting the very disease you're immunizing against. Can provide more on that in round. Other illnesses are also possible side-effects of the virus even when the manufacturing etc is perfect.admin: And I should clarify that the 5% is not necessarily the same 5% or so who receive no measles protection after a dose of the vaccine.admin: Do you believe that adequate nourishment significantly increases the chances of surviving measles?whiteflame: Of course. Malnutrition is practically a disease in its own right, depriving the body of necessary nutrients. A virus has a more difficult time depriving the body of nutrients through its replication when those nutrients are already above the floor level. It's at least partially the same reason why opportunistic organisms can become infectious after a viral infection takes hold.whiteflame: I suppose I phrased that question poorly (though I'll be interested to see your data on that, because it doesn't match my numbers). Let me rephrase: you said in the previous round that the polio vaccine in India had engendered an infectious disease that was separate from polio. Is there any instance of a disease of similar origins resulting from the MMR vaccine? And have there been any documented instances of non-MMR diseases spread by the vaccine?admin: Not on the same scale, but isolated cases do exist. For example, a dirty needle used in vaccination of MMR has given people HIV before. That wasn't the point of the story though. I was just showing that things can go wrong when humans make errors, which is certainly very possible with the MMR vaccine.admin: Has malnutrition been reduced overall in the past 20 years? If so, is it any surprise that death rates from measles have reduced?whiteflame: Based on trends I'm seeing of underweight children and food security over the years, I'm not seeing that trend. Even if it does exist, though, the effect is at least ameliorated by the increased prevalence of obesity, which also causes a number of immunological concerns. I'd say the main reason for the reduction in death tolls is a) much smaller epidemics, and b) improved of medical tools and techniques.admin: So you're saying people have more or less the same nutritional health as 20 years ago? Wow. What about 100 years ago when MMR records began? How far back does your claim extend?whiteflame: I'd like to see your support for that HIV infection. I understand that humans can make errors, but what you were talking about in your post was the incidence of a new and potentially more dangerous disease resulting from polio vaccination. Is there any incidence of such a disease resulting from MMR vaccination?admin: To be clear: the problem in India wasn't the vaccination. The side effects of that were known and documented. The problem was the method of administration. And yes, MMR vaccines have been mis-administered before. It's just never been a massive problem.whiteflame: I'm not making the claim, I'm merely interpreting what I'm seeing. I'd actually say nutritional health is probably worse on the basis of increased obesity, which started surging upward in the 1970's. I have no doubt whatsoever that, worldwide, nitrition has improved in the last 20 years. I don't believe that to be the case in the U.S.whiteflame: Did mis-administration of the MMR vaccine result in any detectable disease that was markedly different from the three viruses themselves?admin: Yes. Any time you poke a needle in somebody there are inherent risks that have nothing to do with MMR. That's in addition to possible complications from the vaccine itself.admin: I deliberately didn't limit my question to the USA because you were complaining about a very small sample size of MMR incidents there, but would you agree that around the world, nutrition, sanitation and healthcare standards have all to some degree contributed to reducing the impact of diseases like MMR? Or do you believe that it is just medicine and vaccination alone?whiteflame: I would agree that improved nutrition has produced a beneficial effect for many societies worldwide with regards to their immune function, and that, yes, this has resulted in a reduced impact of all diseases. I didn't realize you were asking that question, and I apologize for not recognizing it, though it seems like an obvious answer.whiteflame: So you have documented evidence to the effect that this specific vaccine has produced said infection? If so, I'd like to see it.admin: 1 in 3 vaccine injections, including the MMR injection, is unsafe in four out of six regions of the world, which has contributed significantly to HIV and Hepititis (http://www.who.int/injection_safety/toolbox/Miller.pdf). There's more analysis I want to give on this point, though, than is possible to type here.admin: Just to help me draw a graph here - can you name me some countries where you believe that the environment (encompassing all those things I've been asking about) is generally a healthy one? And for comparison, some countries where generally the environment is not that healthy?whiteflame: Healthy: France, the UK, the U.S. Unhealthy: Sierra Leone, Zimbabwe, Haiti.whiteflame: Does that link provide any data on vaccinations done in the U.S.? It mentions that the biggest problem by far is the reuse of needles by health professionals due to severe cost woes. Is this practice occurring anywhere in the U.S. currently?admin: I never said it happened in the US. You might want to qualify some of your questions a bit. That isn't to say it couldn't be a problem. Certainly in the past, before much was known about how diseases spread, injections in the US not unlike the MMR vaccination had similar problems.admin: Alright, final set of questions. Why do you think the price of recieving the MMR vaccine has doubled in the last ten years?whiteflame: That assumes that it has doubled. I'd like to see evidence to that effect before I can answer that question.
whiteflame: I'd say most complicating infections are problematic enough to be significant. Pneumonia would top my list. I would also have a problem with permanent disease states incurred like hepatitis. The major blood diseases would as well, though less so.whiteflame: So the only loss of rights that matters is one in which rights are lost to someone else? On that basis, who are you losing rights to when you get a side effect from vaccination?admin: You are losing rights whenever the vaccination is mandatory. The side effects are irrelevant to the question. There you're losing rights to the government. Rights analysis is about obligations people hold towards one another. To say viruses have human rights is absurd.admin: Looking at pneumonia. If I get measles, what's the chance I will develop pneumonia?whiteflame: Based on the CDC's numbers, 1 in 20 children get pneumonia, though I can't find specific numbers for adults. http://www.cdc.gov/measles/about/complications.html This year, between January and May, there have been 5, which represents slightly less than that. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htmwhiteflame: I guess I didn't get as clear of an answer to this as I'd thought earlier. You now say that the side effects are irrelevant to the question. Are you now saying that those side effects that result from mandatory vaccination are not abrogations of the rights of those individuals who acquire them?admin: Any effects resulting from mandatory vaccinations are abrogations of rights. Even if the vaccine were 100% effective and had no side effects, making it mandatory would abrogate people's rights.admin: Do you agree with the WHO that the best way to avoid getting pneumonia is through nutrition, environmental factors, and getting a flu jab?whiteflame: I would agree that those are beneficial, but insufficient. Measles specifically makes a person more vulnerable to pneumonia. That's actually the same purpose of the "flu jab," which is meant to prevent you from getting influenza, another major virus associated with pneumonia infections. Nutrition and environmental factors can certainly have an effect, but merely changing circumstances for the better is insufficient. It's also not possible for everyone to change those factors.whiteflame: Alright, I'm still confused by your answer. I understand that your view is that people's rights are harmed by mandatory vaccination independent of side effects. What you seem to be saying is that the side effects are a further abrogation of rights. But you said earlier that surrendering rights was the concern. Who are those rights surrendered to?admin: Side effects are not a further abrogation of rights. If somebody chooses between two medications, they do not inherently limit their human rights by choosing one that may have side effects.admin: I guess my point though, is, isn't pneumonia also rather easily treated and prevented, compared to other illnesses?whiteflame: Not always. Pneumonia can be caused by a wide variety of bacterial diseases, many of which require different treatments and not all of which are easily distinguished. There's also the reality that antibiotic resistance is becoming more and more of a problem, and specifically pneumococcal pneumonia has presented with a great deal of concerns in this regard. http://www.cdc.gov/pneumococcal/drug-resistance.htmlwhiteflame: I feel like I'm not getting a consistent answer here. You said "any effects resulting from mandatory vaccinations are abrogations of rights." Now you're saying that side effects are not a further abrogation of rights. Is there something unique to side effects that ensures that they do not represent a loss of rights? Or are you saying that only in the instance where the vaccine is mandated is there a further abrogation of rights that results from side effects?admin: They're not further abrogations of rights, but part of the same abrogation. The vaccine and all its effects abrogate your rights because of the mandate.admin: OK, I'll save most of my analysis on this for my round. Moving on. Why do you think there's a measles outbreak in the US this year?whiteflame: I'd say the likeliest explanation is two-fold %u2013 one, there's a major outbreak in the Philippines, which is spreading to this country, and two, there's a reduced level of vaccination across the U.S. population. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htmwhiteflame: Alright, I think that answer is straightforward, so I'll go with that. Next question: is approaching herd immunity beneficial, even if we don't achieve it?admin: Noadmin: What makes you believe the level of vaccination in the US is reduced?whiteflame: The CDC's data indicates as much. http://deadstate.org/new-cdc-report-thanks-to-anti-vaccine-hysteria-u-s-measles-cases-have-tripled-in-2013/ Individual state analysis has at least been done for Texas. healthblog.dallasnews.com/2014/08/vaccination-rates-for-kids-are-down-rates-of-infectious-diseases-are-up.html/whiteflame: So increased of immunity are not beneficial if they don't reach herd immunity levels?admin: Yesadmin: (can you repost your link? leads to a page not found page for me)admin: (sorry, my fault)admin: OK - just read both of them. What I don't understand is - are those sources not aware that there's been a consistent upward trend in MMRII vaccine uptake since 2003?whiteflame: I'd like to see your source for that.whiteflame: So you contend that a larger portion of the population taking the MMR vaccine isn't beneficial if that population doesn't cause the country to herd immunity?whiteflame: to reach* herd immunityadmin: Yesadmin: Will provide my sources in round. What proportion of people do you think would be the ideal proportion to have immunized?whiteflame: I've already given idealized numbers on the basis of what is required for herd immunity. I recognize that those aren't currently achievable.admin: So roughly 95%?whiteflame: Optimally, yes.whiteflame: So what is the purpose of immunization, then, from your perspective? Does having sub-herd immunity levels of vaccination harm a population, or do you view it as a net 0? And please, explain this perspective with more than a few words.admin: I think it depends on the vaccination. Different vaccinations have different risks and benefits that different people have to individually evaluate; its purpose just like any other medicine. In my own personal evaluation, I don't consider the MMR vaccine to be a good enough medicine to justify its cost.admin: If I were to provide a credible source, in round, showing that the current MMR vaccination rate is roughly 94.5% for all kindergarten-age kids, would you give up?whiteflame: As that is still sub-optimum and we should be attempting to reach that optimum in any case, that point would not force me to surrender. If anything, that would provide proof that it's possible to reach that threshold of 95%, unless you could show that my policy wouldn't increase the number of vaccinated individuals.whiteflame: Alright, but that means you're factoring other aspects into your answer. Imagine that there were no side effects, and that people were choosing to get the vaccine instead of being required to get it. Would you say that there's a benefit to a more substantial portion of the population receiving that optimized MMR vaccine?admin: In terms of public health, there's a benefit. The same kind of argument could be made for eugenics if you factor no other aspects into your answer.admin: So that 0.5% would be enough to convince you that you need to introduce a mandatory program for everybody?whiteflame: Yes. It would tell me that 94.5% of the population would be practically unaffected by the mandate and receive benefits from the subsidies, while the remaining 5.5% would be affected, bringing the country to the level of herd immunity in the process.whiteflame: Alright, that's enough for that line of questioning. Was mandating vaccination for smallpox a net harm?admin: I don't think so. It was an early experiment and a lot went wrong, but ultimately in my personal view the good outweighed the harm. I would defend the right of others to see that differently if they wanted.admin: Do you believe it was OK for Hitler to force-medicate Jews, gypsys etc?whiteflame: No.whiteflame: What makes mandatory medication for smallpox a net benefit?admin: I didn't read your question right, sorry. If it was mandatory it would be a net harm. What makes it a net harm is that it's mandatory. If you're just looking at the vaccine itself, I'd say it was a net benefit because although the vaccine had its problems it cured a really bad threat.admin: Why is it OK for you to force-medicate but not Hitler?whiteflame: ...If you really want a list of reasons, we can go there. 1) I'm not force medicating. I'm not strapping anyone down and making them take a shot in the arm. 2) Hitler didn't force medicate solely under the auspices of public health. 3) The basis for his force-medication was pseudoscience. 4) I'm not singling out racial groups. This list could go on and on, but I'll stop there.whiteflame: Would you contend that smallpox would no longer be a problem today if no one had ever mandated vaccination for it?admin: No. Smallpox was eradicated in numerous countries with no mandates.admin: In your answer, I note that you DON'T say the Nuremberg principle of consent. Do you believe that Hitler violated any medical ethics by failing to obtain consent?whiteflame: Hitler violated multiple codes of ethics, and yes, I'd say that his choice to force people to be medicated entirely against their will without recourse and therefore completely without any level of consent is problematic. I would also say that those moral failings don't appear in my case.whiteflame: I'm noticing that's not really an answer to my question. Would smallpox have been eradicated from the world as a whole if there had never been any mandates that people take the vaccine?admin: Yes. The vaccine wasn't the only reason it went away, and although it definitely helped, the mandates were not required to ensure high uptake.admin: Is it true that your model imposes a cost on people for doing nothing?whiteflame: It imposes a cost on people who negligently put others at risk, so no, I wouldn't say it's for doing nothing.whiteflame: By what means, and please be specific, would smallpox have been eradicated worldwide in the absence of vaccination?whiteflame: (sorry for the double posts... don't know why that happened...)admin: I never said it would, but that the vaccine was not the only reason. It could not have been done without the vaccine, but better nutrition, better public health, improvements to sanitation and a better understanding of the disease all contributed. Would be happy to expand on all that in my round.admin: Does an unvaccinated person really inherently put other people at risk, or is that only if they actually catch the disease?whiteflame: I'd argue that in the case of these diseases, unvaccinated persons cannot reasonably assume that they will never be exposed to at least one these diseases in their lifetimes. These are airborne viruses with a simple route of transmission that anyone but the most isolated persons risks acquiring.admin: Can a government reasonably assume a person will never jaywalk in their lifetime?whiteflame: No. That's why states have laws against it.whiteflame: (I'll get back to asking more questions later. Right now, I'm just interested in seeing where you're going with this)admin: They have laws against it when you do it, they do not presume in advance that you will and punish you for that. Is my understanding of the law accurate?whiteflame: If you would like to argue that the better alternative is to punish people for getting and spreading these diseases, I will be happy to address that, though I'd like you to flesh out how you would apply a similar method to an infectious disease. I don't think the transition is straightforward and that it creates more problems than it solves.admin: I take it then that it's accurate. Are there not laws in force already restricting the rights of people with diseases like measles, such as rules preventing them from going to school?whiteflame: I don't recall any such laws being pervasive in the U.S., nor are they binding for all schools. Such laws would also be ineffective at preventing the spread of disease, only cutting off one route of transmission. I'd say they're incapable of solving for the problem, and their presence only masks the problem.admin: Do you agree that immunization has a 1-10% failure rate? And further, do you agree that staying away from the disease has a 0% failure rate?whiteflame: Yes, though I would say that the failure rate trends towards the lower end. And yes, if you could tell me a way to completely avoid any chance of transmission of these diseases, "staying away from" them would be more effective, if exceedingly unlikely.whiteflame: You mentioned botched production systems for vaccines. How commonly do incidents occur in the U.S. where vaccinations are manufactured poorly, leading to illness/injury?admin: Nowadays, extremely rarely. The chance has been reduced significantly over the past century. As I established in my case, however, the smallness of the chance is actually irrelevant.admin: If somebody has a compromised immune system, would they not avoid people who have measles etc (literally) like the plague?whiteflame: You seem to be making a few basic assumptions here. One, that someone who has the measles is going to present with symptoms that are obvious while they are infectious. Two, that those symptoms are obviously separate from other common illnesses. Three, that they can avoid all individuals who might be sick without placing themselves in a large plastic bubble. And four, that even if they take intense precautions, that they can avoid indirect infections. It is not simple even if one is taking the fewest risks possible.whiteflame: I read the Murphy's Law contention. Why should voters prefer huge impacts that are extremely unlikely to substantial and still likely impacts?admin: Judges should be free to make up their own mind as to whether potential risks outweigh potential benefits for any medication. I'm simply showing science-supported valid justifications also exist for not taking the vaccine. Many will not accept that argument, and that's fine. I wish them well. It's not me in this debate who is trying to force my opinion on other people.admin: What other "common illness" looks like measles or mumps symptoms-wise that an immune-compromised person would NOT want to avoid like the plague?whiteflame: We've been through the symptoms, I don't think I need to repeat them. Yes, an immunocompromised person would want to avoid them as well. But there are two problems. One, this dramatically increases the number of people that those who are immunocompromised have to avoid, making the process all the more impossible. Two, we're talking about basic symptoms like "fever," "dry cough" and "sore throat," which are simulated quite well by several non-disease states. These aren't necessarily hallmarks of disease, and so aren't so simple to recognize as signs of someone to stay away from.whiteflame: Nice jab. Still, could you tell me the most recent date when a poorly manufactured vaccine led to illness/injury in the U.S.?admin: No because the VICP does not usually make rulings as to what exactly was wrong with the vaccine, only whether the vaccine was at fault at all. Usually there's no real way of telling. It's safe to say that it's rare.admin: What's more likely today - that an immune-compromised person will die from a shark attack or that they will die from measles, mumps or rubella?whiteflame: I won't speculate, though if they're immunocompromised, the process of leaving their home, heading to the beach, getting settled and entering the water all present as opportunities to be infected by those around them. It seems rather unlikely that an immunocompromised individual would further compromise themselves by swimming out far enough to put themselves at risk.admin: If they're not willing to go out to sea, assuming that's true, then can we agree that they'll definitely try to not go near people showing symptoms of those illnesses?whiteflame: We can assume what they'll try to do. We cannot assume that they would be capable of achieving it without encasing themselves in plastic.whiteflame: You mentioned that deaths that occur as a result of measles tend to come from complicating infections. How do most die from influenza and the human immunodeficiency virus?admin: They ALWAYS come from complicating infections. Even in immune-compromised persons - the virus itself is extraordinarily benign. The mechanism for death is similar to influenza or HIV when it occurs in that there are complicating infections, but the virus is far less deadly than either.admin: Do you agree that among the 0.3% killed by complications related to measles among infected in the decade before last, there were only (roughly) 0.045% were immune deficient? Do you further agree that in the last decade, 0% of immune deficient persons who have contracted measles have died?whiteflame: I'm not going to agree to numbers without seeing the sources themselves and validating their findings, so while that may be accurate, I would need to see the support behind them.whiteflame: Is it your contention, then, that the complicating factors that accompany these virus infections are not enhanced significantly (especially in immunosuppressed persons) by the viral infections themselves?admin: Not significantly. The enhancement is minor at best.admin: Since you're making the claim that the harm is particularly strong to immunosuppressed people, do you have any statistics that support that claim in relation to MMR specifically from the past two decades or so?whiteflame: I'll be all too happy to provide primary and secondary evidence in the next round that shows that measles, in particular, presents a tremendous risk to the immunosuppressed, and further that it can and does induce immunosuppression. admin: But are these sources statistics from the past two decades relating to MMR in immunosuppressed people specifically?whiteflame: Would you also say that measles does not have a significant immunosuppressive effect?admin: Yeswhiteflame: Would you say that influenza has a higher immunosuppressive effect? And, if so, what differentiates the two?whiteflame: Yes. If these studies did occur before 20 years ago, though, the effects remain the same. We may be better able to address the resulting fallout today, but that immunosuppression still occurs because we have limited or no understanding of the mechanisms involved.admin: Yes, but not much. Their respective RNA and how that causes them to behave is what differentiates them for the most part, as with pretty much any RNA viruses. I kind of don't understand the point of the question.admin: You say the effects are the same as 20 years ago. Does this mean you believe that the environment plays no difference in how the disease affects people, or are you saying the environment is the same today as 20 years ago?whiteflame: "Environment" is a pretty broad term and can encompass a number of very different variables. Of course there's differences in the environment. Whether those differences are substantial enough to dramatically affect disease progression for the majority of the population that gets measles is another story. If it's your view that there's a substantial environmental difference between the 1990's and the 2010's that is likely to do this, then you should make that difference clear.whiteflame: I'm pretty well versed on viral RNAs myself, so I'll go with what you've given me on that front. Has vaccine-derived illness ever been characterized in people receiving the MMR vaccine? Similarly, has there ever been an instance of transmission of a separate disease to patients receiving the MMR vaccine?admin: Yes, quite frequently. A small outbreak of measles from the vaccine, for example, is observed in about 5% of people who get the MMR vaccine. One of the side effects is literally getting the very disease you're immunizing against. Can provide more on that in round. Other illnesses are also possible side-effects of the virus even when the manufacturing etc is perfect.admin: And I should clarify that the 5% is not necessarily the same 5% or so who receive no measles protection after a dose of the vaccine.admin: Do you believe that adequate nourishment significantly increases the chances of surviving measles?whiteflame: Of course. Malnutrition is practically a disease in its own right, depriving the body of necessary nutrients. A virus has a more difficult time depriving the body of nutrients through its replication when those nutrients are already above the floor level. It's at least partially the same reason why opportunistic organisms can become infectious after a viral infection takes hold.whiteflame: I suppose I phrased that question poorly (though I'll be interested to see your data on that, because it doesn't match my numbers). Let me rephrase: you said in the previous round that the polio vaccine in India had engendered an infectious disease that was separate from polio. Is there any instance of a disease of similar origins resulting from the MMR vaccine? And have there been any documented instances of non-MMR diseases spread by the vaccine?admin: Not on the same scale, but isolated cases do exist. For example, a dirty needle used in vaccination of MMR has given people HIV before. That wasn't the point of the story though. I was just showing that things can go wrong when humans make errors, which is certainly very possible with the MMR vaccine.admin: Has malnutrition been reduced overall in the past 20 years? If so, is it any surprise that death rates from measles have reduced?whiteflame: Based on trends I'm seeing of underweight children and food security over the years, I'm not seeing that trend. Even if it does exist, though, the effect is at least ameliorated by the increased prevalence of obesity, which also causes a number of immunological concerns. I'd say the main reason for the reduction in death tolls is a) much smaller epidemics, and b) improved of medical tools and techniques.admin: So you're saying people have more or less the same nutritional health as 20 years ago? Wow. What about 100 years ago when MMR records began? How far back does your claim extend?whiteflame: I'd like to see your support for that HIV infection. I understand that humans can make errors, but what you were talking about in your post was the incidence of a new and potentially more dangerous disease resulting from polio vaccination. Is there any incidence of such a disease resulting from MMR vaccination?admin: To be clear: the problem in India wasn't the vaccination. The side effects of that were known and documented. The problem was the method of administration. And yes, MMR vaccines have been mis-administered before. It's just never been a massive problem.whiteflame: I'm not making the claim, I'm merely interpreting what I'm seeing. I'd actually say nutritional health is probably worse on the basis of increased obesity, which started surging upward in the 1970's. I have no doubt whatsoever that, worldwide, nitrition has improved in the last 20 years. I don't believe that to be the case in the U.S.whiteflame: Did mis-administration of the MMR vaccine result in any detectable disease that was markedly different from the three viruses themselves?admin: Yes. Any time you poke a needle in somebody there are inherent risks that have nothing to do with MMR. That's in addition to possible complications from the vaccine itself.admin: I deliberately didn't limit my question to the USA because you were complaining about a very small sample size of MMR incidents there, but would you agree that around the world, nutrition, sanitation and healthcare standards have all to some degree contributed to reducing the impact of diseases like MMR? Or do you believe that it is just medicine and vaccination alone?whiteflame: I would agree that improved nutrition has produced a beneficial effect for many societies worldwide with regards to their immune function, and that, yes, this has resulted in a reduced impact of all diseases. I didn't realize you were asking that question, and I apologize for not recognizing it, though it seems like an obvious answer.whiteflame: So you have documented evidence to the effect that this specific vaccine has produced said infection? If so, I'd like to see it.admin: 1 in 3 vaccine injections, including the MMR injection, is unsafe in four out of six regions of the world, which has contributed significantly to HIV and Hepititis (http://www.who.int/injection_safety/toolbox/Miller.pdf). There's more analysis I want to give on this point, though, than is possible to type here.admin: Just to help me draw a graph here - can you name me some countries where you believe that the environment (encompassing all those things I've been asking about) is generally a healthy one? And for comparison, some countries where generally the environment is not that healthy?whiteflame: Healthy: France, the UK, the U.S. Unhealthy: Sierra Leone, Zimbabwe, Haiti.whiteflame: Does that link provide any data on vaccinations done in the U.S.? It mentions that the biggest problem by far is the reuse of needles by health professionals due to severe cost woes. Is this practice occurring anywhere in the U.S. currently?admin: I never said it happened in the US. You might want to qualify some of your questions a bit. That isn't to say it couldn't be a problem. Certainly in the past, before much was known about how diseases spread, injections in the US not unlike the MMR vaccination had similar problems.admin: Alright, final set of questions. Why do you think the price of recieving the MMR vaccine has doubled in the last ten years?whiteflame: That assumes that it has doubled. I'd like to see evidence to that effect before I can answer that question. whiteflame: So that price is solely for the MMR II vaccine? Is that price increase consistent with GSK's product, Priorix, as well?admin: Priorix isn't sold in the US. It obviously depends a lot on the market in question, but the general trend has been an increase in price over time. That price is solely for the MMRII vaccine. Given this, can you now answer my question about why the price of getting an MMR vaccine in the US has risen so significantly?whiteflame: I asked my question that way for a reason, I'm just trying to establish something. I think I'm satisfied on that front as well.whiteflame: I can speculate based on my knowledge of the pharmaceutical market and vaccine sales, but no, I don't have a definitive answer.admin: Did you know that when the polio vaccine was invented, the inventor refused to take out a patent, specifically so that as many people as possible could get the treatment inexpensively?whiteflame: Ah, I figured you were going there. Yes, I've heard that story. If you want to discuss the necessity of drug patents, that's a very large and complex issue.admin: Do you think it's fair, in general, for the US government to mandate payments, primarily from the middle class, to a private company making millions in profits for their primarily wealthy investors?whiteflame: I'd say that answer is contingent on a number of factors. I can't say that it's fair in every instance, but I also can't say it's unfair in every instance. I think I've provided a lot of the reasoning already for why society requires this mandate, and I'll be happy to defend it on other levels if you could narrow down the question.admin: Alright then, final question. Is this really the biggest public health issue for the US to solve right now? Like compared with all the other problems the US faces, and mandates they could be making, do you honestly believe the US has nothing better to do than mandate an MMR vaccination?whiteflame: Of course not, though I do think it's a substantial problem that is capable of being solved much more cleanly and clearly than the bigger health issues in the U.S. I'd say heart disease, cancer and diabetes are bigger problems, but they're rather large health problems with no solid solutions. Same for obesity, Alzheimer's, and COPD. Even if these were things we could solve for in some reasonable fashion, I don't see why there's a need to be overly selective in regards to what we're solving for. Whether this is the biggest issue or not, it's still a worthy one.admin: OK then, I look forward to reading your last round! Feel free to ask me any other questions you may have too.whiteflame: I think I'm good. I appreciate the spirited cross-x, Lars. Haven't ever done it before (beyond that one time with RM, which I don't count), and it's been enlightening to me.
whiteflame: So that price is solely for the MMR II vaccine? Is that price increase consistent with GSK's product, Priorix, as well?admin: Priorix isn't sold in the US. It obviously depends a lot on the market in question, but the general trend has been an increase in price over time. That price is solely for the MMRII vaccine. Given this, can you now answer my question about why the price of getting an MMR vaccine in the US has risen so significantly?whiteflame: I asked my question that way for a reason, I'm just trying to establish something. I think I'm satisfied on that front as well.whiteflame: I can speculate based on my knowledge of the pharmaceutical market and vaccine sales, but no, I don't have a definitive answer.admin: Did you know that when the polio vaccine was invented, the inventor refused to take out a patent, specifically so that as many people as possible could get the treatment inexpensively?whiteflame: Ah, I figured you were going there. Yes, I've heard that story. If you want to discuss the necessity of drug patents, that's a very large and complex issue.admin: Do you think it's fair, in general, for the US government to mandate payments, primarily from the middle class, to a private company making millions in profits for their primarily wealthy investors?whiteflame: I'd say that answer is contingent on a number of factors. I can't say that it's fair in every instance, but I also can't say it's unfair in every instance. I think I've provided a lot of the reasoning already for why society requires this mandate, and I'll be happy to defend it on other levels if you could narrow down the question.admin: Alright then, final question. Is this really the biggest public health issue for the US to solve right now? Like compared with all the other problems the US faces, and mandates they could be making, do you honestly believe the US has nothing better to do than mandate an MMR vaccination?whiteflame: Of course not, though I do think it's a substantial problem that is capable of being solved much more cleanly and clearly than the bigger health issues in the U.S. I'd say heart disease, cancer and diabetes are bigger problems, but they're rather large health problems with no solid solutions. Same for obesity, Alzheimer's, and COPD. Even if these were things we could solve for in some reasonable fashion, I don't see why there's a need to be overly selective in regards to what we're solving for. Whether this is the biggest issue or not, it's still a worthy one.admin: OK then, I look forward to reading your last round! Feel free to ask me any other questions you may have too.whiteflame: I think I'm good. I appreciate the spirited cross-x, Lars. Haven't ever done it before (beyond that one time with RM, which I don't count), and it's been enlightening to me.Return To Top | Speak Round
whiteflame (PRO)Alright, thanks again to Con for engaging with me in one of the most interesting debates I've had. I do apologize for the tremendous amount of text to follow – Con gave me a rather long round himself and a large amount to cover from cross-x, and I'm sure his final round will be similarly verbose. Thanks to the voters in advance for taking the time to go through these posts; it may be only two rounds, but with this amount of text, it seems more like 6.
Fundamentally, this is a debate weighing the aggregate utility of the MMR vaccine to public health and the lost liberties that result from its being mandated. The reality is that neither of these should be preferred in every case. I'm not going to sit here and argue that every measure we can take to address a given public health threat is worth the loss to liberty it may engender, nor do I think my opponent would argue that those lost liberties should always outweigh any benefit to public health that could occur. So really, what this debate is about is how we strike that balance, and where MMR comes out when that balance is struck. So there are a few questions that this debate comes down to by the end that need to be thought through as I go through Con's points:
1) Do the MMR viruses present a substantial risk to the public health of the United States?
2) Can that risk be ameliorated to a significant degree by mandating vaccination?
3) Does that risk reduction outweigh the potential loss of rights that accompanies it?
By the end of this round, I plan to show that the answers to all of these questions is an emphatic “yes!” A big part of the reason why is that Con is continuing to treat vaccination as an individual choice on the basis that their purpose is for their own protection. And this is the problem – a vaccine isn't solely meant to protect the person receiving it. Voters, this is the main point you must keep in mind as I go through this rebuttal and conclude; Con's arguments for individual rights just miss the basic point, and treat commonly dangerous viral infections as little more than nuisances without cause.
But onto the rebuttals.
Mass Medication
1. Con does a good job ginning up fear of mass medication without any real explanation of harm. Note that nowhere in this point does he ever state why mass medication is wrong. He says that mass overmedication is harmful, but the sole reason he provides is that it's like eugenics. The problem is that a) he never says why eugenics is wrong, merely insinuating that there's an inherent harm to all of eugenics (recognize that genetic counseling could be considered “eugenics,” as it's also the “practice of improving the genetic quality of the human population”)[15] and b) changing genetic structures, thus altering traits inherent to a person, is substantially different from providing basic nutrients, which only alters what they eat and drink. Con provides no analysis on why any given vitamin shouldn't be packaged more commonly in foods and drinks to improve public health.
2. Most of this has absolutely nothing to do with my case. A person neglecting or refusing to take a vaccine puts others at risk by their inaction, as the spread of a disease to them could consequently increase the chance of its spread to others. If a person neglects or refuses to take a certain nutrient, the harm is solely their own. One could argue that some of these vitamins are important for staving off disease, but the sole diseases that are definitively linked to vitamin deficiencies aren't infectious.
3. The sole piece of this contention that is applicable to my case misrepresents both the purpose of vaccines and my case. In the former case, vaccines are much better as a preventative measure. Yes, vaccines are pursued largely in instances where there are large outbreaks in order to prevent the spread. However, the main purpose is to prevent those outbreaks. The most effective usage of vaccination prevents any epidemic, it's not responsive to one. As for my case, I'd say I'm not responding to outbreaks (as these are usually sporadic in the U.S.), but rather responding to a changing mentality, which has pushed people to fear vaccines that functions mainly on the basis of pseudoscience.
Human Rights
1. This appears to be at least part of the impact story for the previous point, but it still lacks anything definitive. He essentially just asserts that there's a harm to obligating people to receive the necessary medications to be healthy, but never states what that harm is beyond this general assertion of “human rights.” He never provides any specific analysis as to why people should have the right to refuse treatments that are proven to be beneficial to them and those around them. Why is it moral to allow a person to refuse care on the grounds of personal autonomy? It sounds nice, but Con is going to need to provide more than just his assertion that it's wrong, especially when he admits that many schools can and do already require incoming students to be vaccinated, and when many jobs require a wide variety of vaccinations.[16]
2. Con uses the Universal Declaration of Human Rights to support his argument, but never points to anything within it that specifically upholds this principle. If anything, the one aspect he quotes points towards the necessity for each person to have this right to health and medical care, something that's only realistically possible in a world where herd immunity protects those individuals who are most susceptible to these diseases.
3. I take issue with this presumption of guilt argument. I'm not presuming guilt any more than tax policy assumes people are cheapskates. I'm assuming that it's negligent to ignore one's capacity to easily spread a dangerous disease when one has the capacity and the means to prevent it.
4. Con's argument seems to apply to practically any instance in which autonomous actions are restricted for the benefit of the general public. It could just as easily be applied to taxation policies, requiring automobile insurance, and obeying road signs. Con has provided nothing specific to choice of treatment that makes it special, except to equate body autonomy to a nebulous “right to life” that apparently has to be exercised through medical decisions, but can be abrogated in other areas for the benefit of the general public. Why should I be able to “make [my] own destiny” when it comes to vaccinations, but not able to engage in these other risky behaviors?
5. Let's look at the sole example of a vaccination that resulted in eradication of a disease: smallpox. It was mandated for the first time in the U.S. in 1809.[17] It was upheld there in Jacobson v. Massachusetts. The justices compared it to the Civil War, “saying that a community has the right to protect itself both from disease and from military invasion...'there are manifold restraints to which each person is necessarily subject for the common good.'”[18] The British government followed in 1853.[19] These procedures led to complete or nearly complete elimination of the disease over the next century in these countries. People like Frank Fenner are responsible for the eradication of smallpox in Africa, which often went against the will of native populations.[20] And that's not even what I'm seeking here. The alternative of accepting the fine for those who do not wish to be vaccinated, which is also upheld by that USSC decision, makes my case far more reasonable.[18]
If that's not enough, we could take a look at current policies. There are dozens of countries that require the yellow fever vaccine.[21] Saudi Arabia requires meningococcal disease and polio vaccines, mainly because of a large influx of pilgrims to the country.[21] These are recognitions of broad public harms that many countries have agreed need to be prevented using a consistent mechanism, and that mechanism is vaccination.
We're not the same
1. This is generally just an obvious point. Of course we're not all the same. However, each of us is vulnerable to the spread of these diseases on the basis that we are human beings without immunity to them. That doesn't change on a person-by-person basis. Unless you've built up the highly specific antibodies to the virus that you need to combat it, it's exceedingly unlikely that you could fight off any of these viruses before getting any symptoms. People will generate those antibodies and mount an immune response at different rates, changing how long the infection lasts and how strong of any effect it has, and other immune defenses come into play, but to my knowledge, there is no population of humans that is immune to any of these diseases before being exposed to them.
2. My plan would be implemented using doctors' discretion, as that keeps medical records confidential.
3. Con says that there are possible health complications that could result from something that the patient doesn't want to reveal to their doctor. That's true enough, but if the patient is aware of this source of complication, then they can either choose to reveal that to their doctor, or choose to pay the fine. They are not forced to put themselves in a medically dangerous state, and doing so would be their choice. If the patient is unaware of this problem, then mandatory vaccination isn't the concern, but rather a lack of education on the matter is. They would be put in the same danger if they chose to get vaccinated under those circumstances. If they've chosen not to discuss it with a medical professional or look up prescription drug interactions online (they're not that hard to find [22]), then the state should not be deemed responsible for those consequences. The harm is something they brought on themselves.
4. Much of this can still be solved by a basic blood or urine test before vaccination. This doesn't have to be mandatory – it can be linked with vaccination, and patients can sign off if they don't wish to have these tests. This provides them with an option that can further improve the safety of their vaccination, and afford them an opportunity to exercise their bodily autonomy if they wish. It's a way for doctors to ensure that there's no possible concerns in their system, and essentially know them as well as they know themselves in this regard. If a given drug doesn't appear in these tests, then it probably is no longer at perceptible levels, and therefore is not a concern.
5. Note that Con never provides any examples of this happening. An attenuated vaccine of the sort I am discussing is not a chemical. It's virus particles. To my knowledge, there are no dangerous chemical interactions with vaccines. Problems like vaccine overload are the result of excessive challenges to the immune system, and are prevented by ensuring that patients aren't given too many vaccines at once.
6. I'm not sure what's dehumanizing about ensuring a higher standard for public health. Con simply asserts that this is “a ritual activity for the sole purpose of making us more similar,” but that's not even part of the purpose. The purpose is disease prevention, not similarity. You and I will likely have dissimilar reactions to the vaccine and produce dissimilar antibodies to different viral proteins/nucleic acids or different parts of the same viral protein/nucleic acid. I don't even see why medical similarity (or for that matter, any similarity) is inherently dehumanizing. Con doesn't explain.
7. The comparison to tetanus is absurd. Tetanus is not an airborne disease with the ability to spread easily from person-to-person. The whole idea of “liv[ing] healthily” is similarly bogus. If I eat all my vegetables and exercise every day, I'll still be able to contract measles from my next door neighbor if I don't have the vaccine and have never been exposed to the virus before. Con's claim that we “should have the right to decide what means of avoiding sickness is right for” us is entirely empty – the only means he provides are only partially effective at best. Choosing one of them over vaccination represents an unsound decision that puts the well-being of others at risk.
8. I don't understand this argument that not being vaccinated somehow makes you more health conscious. Con barely warrants this statement and says it's, in his own words, “a weak correlation.” That's the best case scenario for him. The truth is that there's likely no correlation. In fact, I would argue that a society that is built around a public consciousness of an ongoing healthcare threat is going to be the one in which more people are health-conscious. Hearing about this in the news and having constant discussions on viral infections and staying healthy is going to inform people of the health risks involved and push them to improve on behaviors that would otherwise be treated as unimportant, like a healthy diet, exercise, and hygiene. This discussion is far less prominent in status quo.
Murphy's Law
1. This entire contention is non-unique to any case that modifies away from the status quo. Murphy's law is essentially an elegant way of saying “shit happens,” a pessimistic comment on how many view the world and anything that happens in it. Actually I take back what I said – if Murphy's law is right, then anything can and will go wrong in the status quo as well, so it doesn't just apply to alterations, but to the status quo itself. And I don't need an adage to show that it is going wrong, not with all my epidemiologic evidence. Con will need to provide some exceptional support for his statement here to match that. All he's done is express a generalized negative view with insufficient warrants.
2. The reality is that Murphy's law is incorrect, and it doesn't take much in the way of examples to show this. When the Space Shuttle Challenger exploded, NASA quickly figured out the culprit was the O-rings that had already been under suspicion in 25 previous Shuttle missions. If we run with Murphy's law and its implications, those flights should have blown up as well. They didn't, but they also didn't pass on their lessons, as engineers already knew that charring and hot-gas “blow-by” were problematic in these previous missions. That failure is what led to theChallengerexplosion, not Murphy's law.[23]
3. Moreover, the U.S. has learned from the past – we have disposable needles, we have the Food and Drug Administration and the Center for Biologics Evaluation and Research as a monitoring agencies, and we require multiple quality controls and assurances to be certain that vaccines are safe. Past sources of harm are now vanishingly small concerns. These aren't O-rings, they are problems that have been addressed.Con has basically built this entire contention on a very low probability set of outcomes that, I would argue, are negligible in this debate. We could discuss doomsday scenarios all day long (like how every human being these diseases get into is a possible source of mutation into something extremely deadly), but what we're concerned with is likely outcomes. Con needs to show that the risks he's presenting for the MMR vaccines are a reality, not just claim that they're part of some possible dystopian future. He can't just assume that the risk is present solely based on the existence of human fallibility, especially when he cannot present a single instance of botched vaccine production in the U.S., fails to present any examples in the U.S. that support the incidence of unique disease resulting from vaccination or any transmission of separate disease by vaccination here, and claims a false incidence rate of these three diseases resulting from the vaccines.[24]
4. Con discusses the possibility of adverse reactions, actually providing some of my rebuttal for me through the VICP. However, that's not all. According to the Vaccine Adverse Events Reporting System (VAERS), there have been just over 6,000 adverse events associated with MMR between 1990 and 2012.[25] That's with much of the population receiving these vaccines. One might notice that it attaches a death toll onto that as well, which I'm sure Con will attempt to belabor. However, that misses the reality that these deaths have never been linked directly to taking the MMR vaccine, especially given an extensive (1.5 million person, 11-year) post-marketing, controlled surveillance study that showed no deaths or permanent damage.[26] Con will no doubt point back to Madyson Williams, but this will do him no good, as the problem here was that she had taken two live virus vaccines – MMR and varicella zoster – at the same time, something advised against by Merck itself, partially for this reason.[25] Also note that the age of the child was just 1 year, and that the majority of the VAERS-reported issues occur among children of 3 and younger, none of whom are required to take the vaccine at that age. Doctors can and do recommend that this should come later in life.
In any case, Con will have to establish a scientifically sound link between MMR vaccination and a death toll if he wishes to prove this. Merely pointing to past failures of adherence to clear guidelines is insufficient, as is his correlative analysis of the more severe side effects of taking the vaccine. I've shown a causal relationship between getting these viruses and the outcomes I've described, he will have to show that same relationship between the vaccine and its purported outcomes. While vaccines have and will continue to become safer, these diseases will continue to be extremely dangerous to the immunocompromised, as well as the very young and old.
Still, that's 6,000 adverse events over 22 years, and while most of those may not have been caused by the vaccine itself, those events are still worrisome. Let's compare that to the harms I cited for these diseases earlier. With 3-4 million people infected by measles, 48,000 were hospitalized, 1,000 developed chronic disabilities, and 400-500 deaths occurred. That's 1 in 84, 1 in 4000, and 1 in 10,000, respectively. 10% of patients with mumps end up with meningitis, and 1 in 2000-30,000 cases develops hearing loss. Out of 12 million cases of rubella, 20,000 suffered complications. That's 1 in 600. Notice how each of these numbers is far higher than the 1 in 300,000 and 1 in 1,000,000 my opponent provides. Something goes wrong far more often with these diseases than it does with the vaccines.
5. Con points to the possibility of a botched production system, but seems to have little knowledge of how a vaccine is approved and just what procedures a company has to go through to produce, store and deliver a vaccine. They have to be manufactured consistently under current good manufacturing practices (cGMP, which you can find extensive details on here [27]), each product characterized, and lots are tested before release to the public.
Con backs this claim up with the bold assertion that smallpox vaccines were once contaminated with syphilis. What he fails to realize is that a) this only occurred during the days of arm-to-arm transfer, b) it occurred well before scientists developed the basic molecular detection systems used today to screen vaccines, and c) is only occurred in 750 cases out of 100 million vaccinations, making it incredibly low likelihood.[28]
Con's second attempt to back this claim is through the example of India in 2011. This is flawed as well. Con will need to show evidence that the MMR vaccine leads patients to shed communicable and virulent virus, something he has so far failed to do. The few sites that I can find arguing that this is the case are all strongly anti-vaccine, and lack any proof to support their assertions. Con is also comparing two very different countries with very different circumstances. India suffers from “poor sanitation, including open sewage in underdeveloped countries, where drinking water is too often also used for bathing and disposal of human waste,” which “can make it easy for vaccine strain polio virus to be transmitted...especially among those, who are immune compromised, malnourished or suffering from serious health problems.”[29] Not only does my model not take place in India and therefore doesn't suffer nearly so greatly from these problems, but it would allow many of those who are most seriously affected outs from getting the vaccine, not to mention ensure that they are less likely to contract these illnesses in general. Even Con admits that there are substantial differences between the two countries in terms of quality control, but he understates those differences markedly.
6. I would argue exactly the opposite – botched batches of vaccines are far less likely in a country where vaccination is required. Many of the groups who are anti-vaccine are likely to launch extensive campaigns to make sure what they are taking is not contaminated, and measures by the FDA are likely to be stepped up to ensure that companies like Merck put out the best quality stuff. A failure on the part of the FDA or any of these companies would be a dramatic harm to either one, and so they would endeavor to prevent such errors to the greatest extent possible.
7. Generally, I disagree with the way my opponent phrases his disagreement with my case here. He says that taking a vaccine is “putting their body on the line and gambling with their health,” but he hasn't proved that MMR creates any substantial threat, focusing instead on other, unrelated diseases and low-risk impacts. The idea that “people are [going to be] force-killed by the government” is simply Con trying to make it sound far more dramatic than it is. He will have to do more than quote Murphy's law to make this stick.
MMR: The Diseases
1. By Con's logic, no one ever died of HIV either. This is just a ridiculous point – most illnesses don't kill people by themselves. Death is the result of multiple illnesses, but the immunosuppressive effects of one are often necessary to allow the others to infect. Since measles can't be cured by medicine, there is a severe problem here that can't always be cured by Gran Turismo. If a person's immune system is not capable of defeating the virus, then it can easily lead to complications. Coca-Cola and “getting comfortable” aren't cures or treatments, just ways to ride out light symptoms.
2. Con has a rather large burden that he's building for himself here by claiming at these diseases are minimally important. I've shown that, yes, even rubella has terrible consequences for pregnant mothers. I don't think that it's reasonable to put any of them at risk of contracting this airborne disease. I showed that mumps causes meningitis, which can read to a number of neurologic symptoms, as well as encephalitis and even hearing loss. Con ignores orchitis as a plausible harm as well, something both of us could easily appreciate. Con similarly ignores every complication beyond death for measles, which results in a tremendous number of hospitalizations and an admittedly smaller number of chronic disabilities, as well as numerous serious complications that I listed.
3. I don't need to present a disease with a high death rate to show that vaccination is worthwhile. I've already explained how damaging each of these diseases is to large populations, and what complications can arise. The fact that they're not significant enough for my opponent to care doesn't make them insignificant. If anything, smallpox showcases just how effective a program like this can be. There may be other diseases that are more deserving of these efforts, but all of them (including tetanus) aren't easily transmissible between patients.
Nonetheless, Con is entirely right that the most common symptoms of these diseases is akin to the common cold. Unfortunately for him, that's a big problem for Con's case. What this means is that most people will treat them like a cold – some may stay home, but many will go out and fight through their illness, treating it like a minor impediment to their day. This is why diseases like Ebola are insidious – most of the symptoms one experiences early on don't look like anything special: basic headache, fever, and muscle pain, which one might attribute to having a bad day and perhaps an early flu. It's during these early symptoms, and not the excessive bleeding stages, that one is most likely to spread the illness. At this stage, they're contagious, and it's not obvious what they have. People experiencing these symptoms would be tempted to just walk it off, and would thus continue their usual interactions. This is all the worse for MMR, where most people never experience the more damaging and obvious complications, and therefore may continue to spread the disease over the entire time they're infected.
Maybe Con would stay home if he's infected, but many would just try to move on with their day. Unlike Ebola, these diseases have less common complications. However, also unlike Ebola, they're highly contagious to everyone sharing the same space, especially if it's enclosed like a subway train or crowded office. Avoiding direct contact isn't enough, as these diseases are airborne. The chances of them spreading broadly are far higher, putting more people at risk of developing these complications.
In America!
1. The fact that Con can present problems with our health care system is non-unique – every system has problems (and incompetent doctors, for that matter), and he hasn't shown these to be excessive or pervasive, only providing evidence of an audit that found unspecified “inconsistencies” in the system, and those only appear to be in regards to information submitted online. He doesn't show any actual problems with Obamacare as a system, just claiming that the failures of data submission reflect huge problems with the system as a whole.
2. I don't understand the choice to lampoon Obamacare, as it has nothing to do with my policy. Implementation is done by the health care professionals doing it, not how insurance is provided.
3. Con never actually shows where the problems are that would affect implementation. He says “there's probably something wrong somewhere,” but that doesn't suffice as proof that my system will fail, in part or in totality. He points to 4 doctors who are not currently practicing in public health nor at all likely to participate in the distribution of vaccines, and then claims that they're representative of how terrible our public health care system is. If, as he claims, “they won't be able to pull this off perfectly,” then Con has to state specifically where the deficiencies are, how they are likely to affect the system, and how that will lead to failures. He can't just generalize this and say that he doesn't know where, he doesn't know when, he doesn't know how, but something bad is going to happen.
4. Failures of public health occur now with regards to controlling outbreaks like those resulting from these viruses. There have been multiple outbreaks involving hundreds of people over the last several years. Those failures far outdistance any of the probable failures with regards to vaccination.
5. Con never warrants his predictions, particularly on the cost issue. Either a lot of people will pay fines, a lot of people will be vaccinated, in which case health costs (for diagnosis, treatment, quarantines, epidemiological tracking, etc.) will decrease, or it will be some permutation of the two. In any case, these ameliorate if not eliminate cost burdens.
Brief Rebuttals 1: Herd Immunity
1. I didn't realize I needed to link the numbers to the suffering experienced by those numbers, but I'll do the basics. The human body normally exists in a homeostatic state, meaning that the system is regulated to a stable point. Viruses like these chuck that state into uncertainty by causing disease, and cause people harm. Whether that harm is through the basic fever, chills, stuffy nose, cough, etc., or if it's through more dramatic complications like encephalitis, there's an objective harm to experiencing them, though how bad the experience is is subjective. Nonetheless, we can make rational assumptions about what is a worse experience for victims of a given disease and make conclusions as to how strongly those experiences affect them. This is a utilitarian argument – health and wellness are better for society than disease.
I'd say that this suffices as a strong link between the science and the morality – individuals may be able to select for themselves which experiences they will willingly engage in, but they should not be able to make those decisions for others, let alone strangers. When disease spread can be reduced or eliminated, utility says that that public health outcome should be preferred.
2. I'm glad my opponent and I agree that the link between MMR and autism has not been established, and that it is therefore unimportant to this debate.
3. Part of the problem here is that Con's making assumptions based on what I've said. The reason why I don't believe herd immunity is possible is because I think it's likely a substantial portion of the remaining population will choose to pay the fine or manage to avoid the law. However, going off Con's own claim that 94.5% of the population is vaccinated (as he hinted in cross-x), then this makes it very much a possibility. Con's link shows that 95% of vaccines are effective against measles, 96% are effective against mumps, and 99% are effective against rubella, and that's just the first dose.[26] Taken together, that might lead to the figures Con claimed, but then, this ignores the second dose, which induces an immune response in 99% of recipients.[27] If the numbers are as close to 95% as Con seems to believe, then my case could certainly achieve herd immunity with those numbers.
4. Con assumes that outbreaks will never become more substantial than they have been over the last few years. The data bears out a very different trend.
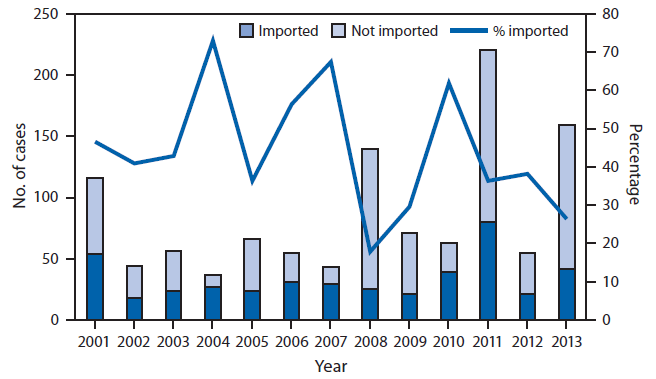
Note that, in years with substantial epidemics in other countries that lead to large amounts of imported cases. The larger the amount of imported cases, the larger the outbreaks in the U.S. The size of the outbreaks in the U.S. have increased substantially as well by comparison in recent years, revealing a widening disease spread.
In case that's not enough proof, we can see the trend playing out this year as a result of a large outbreak in the Philippines.[30] The point being that any epidemic abroad threatens to do tremendous harm in this country, and those epidemics aren't going away anytime soon. Since the level of protection in the U.S. appears to be going down, which I would argue is the result of reduced vaccination levels. While the country as a whole appears to have a vaccination rate among kindergarteners of 94.5%,[31] the vaccination rates in many states are well below that number, with 5 states (Colorado, Arkansas, Pennsylvania, Idaho, and North Dakota) below 90%.[32] In case that's not enough proof that the trend is downward, here's a CDC report to that effect, as well as a study showing that vaccination rates are down in Texas.[33, 34]
5. Con makes the argument that cost of allowing these diseases to run rampant is lower than the cost and impact of preventing it. Con's own link, however, doesn't bear this out. The link points to the Haemophilus influenzae and Pneumococcal vaccines barely reduce the incidence of these bacterial diseases, are expensive, and put those who take them at substantial risk. I agree on both fronts, but these do not apply to the MMR vaccine. The article itself only mentions measles once, and does so in the context of “the 6 basic vaccines” that they deem at least as beneficial.
6. If Con had wanted to present a counterplan regarding feeding starving children, he could have. All he's done here is present it as a nebulous alternative to the putative costs he sees as coming from my case. The reason he didn't is probably because it's not mutually exclusive to my case. We can both mandate immunization and improve governmental programs aimed at feeding starving children. He provides no reasoning for why U.S. resources are so scarce that we can't do both, especially when he hasn't proven that there's any deficit of funds resulting from my policy.
7. Note that Con's chart solely addresses the mortality of measles in England and Wales, not its incidence. I agree that mortality has reduced due to a variety of factors that have changed since the early 1900's. There has probably been a reduction in measles outbreaks as well resulting from those factors. But I would argue that this can only take us so far, and that we're basically at that point already, yet we're still experiencing major outbreaks that correlate strongly with reduced immunization and outbreaks from other countries.
8. Con argues that non-immunized children have mild infections. His data comes from India, so it seems difficult to apply to the U.S., but if we did, this would be really problematic for his case. It shows that there are likely many sub-clinical infections in the U.S., which could easily be prevented from spreading by the vaccine. Con might see this as a sign that measles is effectively harmless in the majority of those infected, but this only lasts so long as they have sufficient immunity to ensure that the virus doesn't transition from a latent stage (where cells are persistently infected, but lie dormant) to a lytic stage (where there is active virus replication an d spread, resulting in cell death). If the immune system is sufficiently challenged by practically any other infection or sufficient injury – hell, even depressed by a strong bout of anxiety [35] – these patients can experience full-blown, infectious measles as a result. All Con has managed to prove here is that the generated resistance that results from getting the infection is often insufficient, leaving open the possibility for viral reactivation. Preventing the infection from becoming latent in the first place only becomes a near certainty with the vaccine. Note that the link also showcases only a 2% measles contraction rate following vaccination, which shows that the vaccine is 98% effective at preventing the infection.
9. Con's point that it may not last a lifetime, is really just mitigation. We're still talking highly likely, long-term resistance to infection.
Brief Rebuttals 2: The Impact
1. Con just seems to use much of his rebuttals here to distract from the issues at hand, and he starts it off with several fallacies. First, there's an appeal to the emotions of the voters, even going so far as to say that his points here should breed anger. Of course, he never gets around to discussing the impacts of any of these bans, assuming that they're harmful solely because they make us angry. Then, he engages in a slippery slope fallacy, emphasizing how the idea of protecting everyone from everything is problematic, and failing to provide any analysis of how my case leads to this extreme and peculiar outcome. I've made it quite clear what makes MMR dangerous, and why it is an important concern. My case doesn't include any of these bans, nor would they be organic offshoots of my case.
Finally, Con engages in an appeal to ridicule, essentially stating that I'm “scaremonger[ing]” and that my argument is an attempt to paint vaccines as supernatural. Maybe he's just talking about others who hold similar views to mine, but this is still meant to paint my argument in an absurd light with no reasoning. Presenting the data as I have isn't scaremongering. I'm making basic conclusions from the data I've presented and provided both the data and conclusions for my opponent and the voters to peruse. I'm not treating vaccination as “a magic cure-all,” and I don't appreciate that kind of embellishment of my case for Con's benefit. I'm not making claims I can't support about what the vaccine does. What these “vaccine lobbyists” Con discusses have done has no bearing on my argument. Con seems to simply be attempting to malign my case by making it sound like I'm peddling snake oil, despite recognizing that it's not earlier in his post. There's no magic here and no attempts to scare people into submission (an interesting take from someone who used several appeals to emotion).
2. Con points to a number of possible medical concerns that could come from everything from the common cold to smoking to eating cake. It is not my burden in this debate to show that these things are insufficient concerns to warrant further action. I will, however, address Salmonella, as he spent a good deal of time there.
He starts by talking about an imaginary vaccine that specifically addresses toxins made by Salmonella, assuming all the responses that would come from it.
First off, just the absence of Salmonella toxins wouldn't mean the absence of disease.Salmonella could still infect you, still alter your gut microbiota to the point that you suffer ill effects, still deprive you of many beneficial nutrients, and, without the toxin, would take longer to clear from your system (the toxin is there to ensure that it gets excreted).
Second, there are multiple toxins coming from two different species, “six subspecies and innumerable serovars.”[36] Any vaccine would only address a subset of these.
Third, there are a large number of diseases that can also come from uncooked chicken that wouldn't be addressed by this vaccine. These include, but not limited to, Campylobacter, various Clostridia, and Staphylococcus.[37] So even ifSalmonella was completely addressed, eating uncooked chicken would be dangerous.
Fourth, there already exist best practices for reducing the incidence of these infections since they are solely ingested and can be killed by cooking. This isn't spread simply by contact between individuals who are infected and those who are uninfected.
Fifth, it's not my burden to defend every single instance of vaccination. I'm defending a single one, and I'm limiting its applicability mainly on the basis of how it is transmitted, not how potent its symptoms are. That's because one person presents a risk to another, rather than a piece of chicken. Distinguishing the two is important, as your ability to choose what happens to you medically is different from your ability to make a medical choice that can directly affect others.
Sixth, Con never actually presents a harm to doing this, so even if it is somehow a consequence of my policy, he never points to any specific moral concerns that arise as a result. Why would mandating this specific vaccine be problematic? He might say “loss of freedom bad,” but that's not enough of an answer. Freedom in this case is, at best, a nebulous benefit and cannot compare to the benefits of protection against a potentially deadly disease.
3. I take strong issue with the following statement made by Con (and no, saying it in all caps doesn't make the point better):
“MMR vaccines may have reduced the incidence rate, but they have not reduced the harm. THE HARM HAS BEEN REDUCED INDEPENDENTLY.”
The only harm Con has proven has been reduced independently is death tolls. Yes, that harm has been reduced, just as the harm for any illness or disease state has been reduced by the advent of indoor plumbing, better nutrition, less poverty, and dramatically improved medical care. But the problem here is that Con can't just assume that these independent factors are sufficient for erasing the problem, as he has argued in the previous round and repeatedly in cross-x. The complications still happen in countries with the best possible circumstances, and the basic disease states are still the same. Cross-apply this to all the times Con mentions nutrition.
Points stemming from Cross-X
1. Con often argues that there are other effective preventative measures, but each of these is just a mitigating factor. The best he's managed to prove here is that these diseases have vastly reduced effects in the U.S. as compared with the third world. He's right, but my case has shown quite clearly that the effect is still substantial enough to matter. Con would have to show that these diseases are effectively of null importance in order for this point to win him the debate.
2. Con never really explains his view that increasing levels of vaccination are essentially worthless without actually reaching herd immunity, though from cross-x, that seems to be his contention. I don't know how he could defend this. He says that herd immunity is potentially beneficial because of a reduced spread of disease (the likelihood of spreading it to less than 1 person). He doesn't say why it's beneficial or negligible that that number increase above 1 to a significant degree, as is the case in the states I listed. It seems obvious to me that reduced spread of disease is generally beneficial because less disease/complications is beneficial – Con hasn't argued that it isn't. It seems obvious to me that the more people who are vulnerable to a given disease, the more likely they are to get it and come into contact with a person who is immunocompromised and therefore far more likely to suffer complications – Con hasn't argued that that isn't the case. He'll need to explain and warrant this view if he plans to win it.
3. Con can't reasonably claim that everyone should adhere to his views of what is and is not damaging to their rights structures. Just because he thinks that one can only lose their rights in the instance where those rights are taken and abused by another person or group of people doesn't mean rights can't be lost in any other instance. I would argue that governments have a duty to ensure that their people don't suffer, and that the reason that duty exists isn't just utility. A person can take your rights by coughing on you and transmitting his/her disease, even if they garner nothing from it. A virus can take your freedoms from you by forcing you to stay home for several days or putting you in the hospital. Con's argument that there's essentially no rights lost in these instances seems strange when someone's freedom of action is very much threatened by both the person and the virus involved. Con's entire argument for why mandatory vaccination is harmful to our rights is based entirely off of a similar loss of freedom.
When Con said in cross-x that side effects from vaccination are “part of the same abrogation” of rights caused by requiring those vaccinations, he's essentially admitting to this. He says that they are “not further abrogations of rights, but part of the same abrogation.” I'm still not quite certain what he's trying to do with this, but I can only interpret this one way. He's saying that the abrogation doesn't increase as a result of the side effects, in which case he's simply erasing any rights loss disadvantage that he might have garnered here because it's a part of the same rights abrogation caused by mandatory vaccination. In the process, he's still saying that this is a part of a rights abrogation, which it cannot be without being a rights abrogation itself. He's therefore admitting that the harms of disease do contribute to rights losses, thereby admitting that there's a rights loss that results, while just trying to wave it away as unimportant by comparison. Maybe that's not his goal, but that's certainly how it appears. If he attempts to gain any sort of rights loss from side effects, though, he's effectively admitting that a similar rights loss occurs as a result of illness of any sort.
However, even if you agree with Con that there's no rights loss here, there is most certainly a loss of bodily autonomy, which is the whole basis for Con's contention regarding the rights losses from mandatory vaccination. If loss of bodily autonomy is a harm in and of itself, as Con insinuates, then a disease is the more insidious harm, lacking any alternatives and requiring a substantial and physically demanding sacrifice.
4. While we can establish the physical impact of a disease, we cannot establish that, for all people, each physical impact is just as harmful. Con often tries to brush off a day or two in bed, a fever and a cough, yet each of these requires that the person be out of work for a certain period of time, that they not interact with family members or friends, or that they miss important social events. The impact of even the lowest levels of disease is something that Con cannot assume is so small as to be insignificant.
In fact, Con seemed to spend a lot of time in cross-x trying to show that these diseases have low death rates in the U.S. The truth of the matter is that they do have low death rates, though Con makes no efforts whatsoever to show that complication rates have substantially reduced with time. The complications I presented in R1 are still very problematic, with ear infections in 1 out of 10 and pneumonia in 1 out of 20 children.[38]
If Con's concern is that these complications aren't common today, I showed evidence in cross-x that shows that any change in their incidence has been minimal. And that's not just for pneumonia – hepatitis and blood disorders like pancytopenia and thrombocytopenia are also appearing, even in the relatively small populations being infected.[39]
This isn't a small issue, though I'm sure Con will attempt to characterize these diseases as unimportant as well. Pneumonia is anything but, resulting from a wide variety of possible causes ranging from bacteria to viruses to fungi. This means that they have to be specifically diagnosed before they can be treated effectively. It is still the leading cause of death among children, the vaccine is minimally effective, and, like all bacterial diseases, the bacterial pneumonia is causing tremendous concern as a result of the antibiotic resistance it's generating (most notably with regards to Streptococcus, Mycoplasma, and Klebsiella-caused cases), making other forms of treatment far less certain.[40] In case that's not enough, the spread of bacterial pneumonia is also associated with more severe symptoms in adults as well (often with Klebsiella), meaning that each infection enhances the other.[41] These bacterial diseases play at least as large of a role in the deaths of those who are infected with measles as nutrition (along with many of the basic symptoms of immunodeficiency caused by measles, like peripheral lymphopenia and T-cell depletion).[42]
5. Con is wrong on the immunosuppressive effects of measles.
“[Measles virus] infection produces an immune system paradox. MV infection, while inducing lifelong immunity, also suppresses the immune system leading to an increase in susceptibility to other, secondary infections.” This article actually includes quite a bit of the data that supports this, as it's essentially a review of numerous primary research papers that established this immunosuppressive aspect and several models for immunosuppression that I won't describe here. Just to give a basic idea, though, of what infections can and do occur:
“Secondary bacterial, protozoal, or viral infections occur because of immunosuppression by MV infection. These infections can result in pneumonia, chronic pulmonary disease, otitis media, laryngotracheobronchitis, adult respiratory distress syndrome, hepatitis and diarrhea.”
These are admittedly more common in underdeveloped countries, but less common doesn't mean non-existent in the U.S. This data are still pertinent here.[43]
I mentioned influenza in cross-x. The reason I did that is because much the same concerns exist with regards to this disease, which has caused one of the most, if not the most, severe pneumonia pandemic in world history. Con may want to write that off as unique to influenza, but this is the kind of immunosuppressive effect measles has as well.[44]
Con is similarly wrong regarding the effects of measles on immunosuppressed individuals. He says that it's a minor enhancement. That isn't held up in the literature, where these individuals are far more likely to suffer terrible complications.[45] I can't find a free copy of this study, but it's outlined pretty clearly in the abstract. There are numerous other studies that support it as well, making it clear that complications, including death, are far more common among these individuals.[46]
If you need a list of the types of people put in danger, here's a list: those undergoing chemotherapy and/or radiotherapy, those with organ or bone marrow transplants, those with high dose steroids, those with HIV, and those with severe combined immunodeficiency.[47] All of these people present with substantial concerns, and they can't just “avoid people” with the illness, especially when Con himself presents data that a large proportion of the population infected with the virus carries it at sub-clinical levels, but may still be shedding the virus. Hell, considering how many times I'm using Con's source, I think I should really include it in my citations.[48]
5. Con is just blatantly wrong regarding his view that scant few of those who become infected with measles will experience complications, and he proves this in the last section. He shows that a great deal of measles infections are never cleared from the body.[48] That means that some 30% of patients are infected for life, and in the process, they're put at great risk every time their immune system is depressed. This is a huge problem, since this means that for this subset of the population, they're especially likely to experience the complications of the disease at some point over their lives any time they're immunosuppressed.
6. Con makes the claim that mandatory vaccination was not necessary in order to eradicate smallpox, a disease that he admits in his previous round was one of the biggest scourges of human society. This is a completely unwarranted and entirely false statement, providing no evidence for other methods by which smallpox is consistently prevented from infecting others. The symptoms of smallpox may have improved and its spread may have reduced, but we're talking about elimination here, and of a very deadly disease that spread very rapidly. And this is a disease that was primarily spread in a similar manner to MMR, through airborne transmission. It is factual that mandates occurred in many nations, including a number of African nations, and were instrumental in the elimination of the disease. Use of vaccines would have been far too minimal in many African nations to accomplish such a goal. Much as I disagree with the methods used to enforce this particular mandate, and I'm not arguing for international enforcement, the effects speak for themselves.
The eradication of a disease is of no small importance, and in this case, I'm addressing 3. Con is entirely right that “every infected person infects about one other person on average.” Even if the U.S. doesn't manage to get below 1, getting as close to it is a start to a trend of elimination worldwide, and if the effect does occur, even just in the U.S., the benefits there are stark. Disease eradication means minimal disease resulting from these viruses and little to no need to dedicate resources from control programs like the CDC or NIH (and therefore to put those resources towards other issues). This article even shows that we could save as much as $4.5 billion as a country if vaccination were able to be discontinued in the U.S. as a result of the eradication of measles alone, and other industrialized nations could save hundreds of millions “if measles were eradicated, even assuming that measles vaccination would continue.”[49]
Voting issues:
I know it's been a long round, so I'll post those questions I started out with again to ground it.
1) Do the MMR viruses present a substantial risk to the public health of the United States?
I've shown that these 3 viruses represent a systematic threat to our utility through our public health, that that threat is growing and very likely to continue doing so, and that it persists most strongly in a society that is further away from herd immunity. Whether it's the viruses themselves that cause the harms or the complicating and difficult to treat infections that commonly accompany them, these are diseases that present with exponentially higher dangers as the number and size of their epidemics continue to grow.
2) Can that risk be ameliorated to a significant degree by mandating vaccination?
I've shown that vaccination is the most broadly effective means of lowering the risk of infection and, therefore, both the short- and long-term harms of that infection. Any other means merely delays complications and places many others in danger of more severe outcomes.
3) Does that risk reduction outweigh the potential harms that accompany it?
I've shown that there are rights issues on both sides of the house in this debate, and that the rights arguments presented by Con fail to present any meaningful impacts that can be weighed against those I have provided. I've shown that vaccination presents a minimal and comparatively negligible risk to those who receive it under the stated guidelines, and that any outcomes for societal perception of health are likelier to be beneficial than harmful.
Based on these three questions and their answers, I've shown why you should vote Pro. I now yield the floor to Con to finish out the debate.
15. http://en.wikipedia.org/wiki/Eugenics
16. http://www.cdc.gov/vaccines/imz-managers/laws/state-reqs.html
17. http://www.immunizationinfo.org/vaccines/smallpox
18. http://en.wikipedia.org/wiki/Jacobson_v._Massachusetts
19. http://en.wikipedia.org/wiki/Smallpox
20. http://www.nytimes.com/2010/11/26/world/26fenner.html?_r=0
21. http://www.who.int/ith/vaccines/en/
23. http://ieeexplore.ieee.org/xpls/abs_all.jsp?arnumber=993764&tag=1
24. http://www.kidshealth.org.nz/measles-immunisation
25. http://www.nvic.org/vaccines-and-diseases/Measles.aspx#Injuryv
26. http://www.merck.com/product/usa/pi_circulars/m/mmr_ii_pi.pdf
27. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/Manufacturing/ucm169105.htm
28. http://en.wikipedia.org/wiki/Smallpox_vaccine
29. http://articles.mercola.com/sites/articles/archive/2012/08/28/polio-eradication-campaign.aspx
31. http://www.cdc.gov/nchs/fastats/immunize.htm
32. http://www.advisory.com/Daily-Briefing/2013/08/08/The-states-with-the-best-and-worst-vaccine-coverage
35. www.publichealthreviews.eu/show/p/92
36. http://en.wikipedia.org/wiki/Salmonella
37. http://healthyeating.sfgate.com/risks-undercooked-chicken-2327.html
38. http://www.cdc.gov/measles/about/complications.html
39. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6322a4.htm
40. http://www.cdc.gov/pneumococcal/drug-resistance.html
41. http://www.ncbi.nlm.nih.gov/pubmed/10065681
42. http://www.academia.edu/1462060/Factors_associated_with_fatal_cases_of_measles
43. http://www.ncbi.nlm.nih.gov/books/NBK2487/
44. http://www.nih.gov/news/health/aug2008/niaid-19.htm
45. http://www.ncbi.nlm.nih.gov/pubmed/1538561
46. http://cvi.asm.org/content/13/4/437
48. medind.nic.in/ibl/t03/i1/iblt03i1p8o.pdf
49. www.cgdev.org/doc/millions/MS_case_1.pdf
Return To Top | Posted:
admin (CON)


"the next time a media article blames the “anti-vaccination movement”, or uneducated parents, do a little more research. And remember: people used to think the world was flat, people were imprisoned for suggesting that the earth revolved around the sun (instead of the other way around), and doctors used to doubt the relationship between tobacco and disease."
- A problem
Pro had to show that measles was actually problematic. At best he showed that it may be problematic in some parts of Africa and historical US, but not present US. Or if you're being really generous to pro, you might say he showed what would happen if vaccines were to disappear, but nobody is suggesting that in this debate, and that ignores my mountain of scientific evidence that it's the environment that affects measles health outcomes the most. He mentioned herd immunity but never proved why it was desirable when health impacts are already so negligible. Pro failed to show that the status quo had a significant enough harm. - A solution
Even supposing his problem had stood up, pro failed to show a coherent model to solve that problem. I think in this second round I counted five times where pro changed their model to add in more things as he realized the problems I was pointing out, but it's still fraught with loopholes and difficulties. Notably, he never actually was able to tell you how his model would actually work in terms of checking whether somebody had the vaccine or not - which I would consider probably the most important part to get right. - That the solution solves the problem
Obviously since pro had neither a solution nor a problem. His tenuous attempts to link his solution to his problem have failed and seemingly relied entirely on a small sebsection of the population who are the most vulnerable - without recognizing that these were also the most careful, too. His consistent overestimation of the harms of these illnesses made this difficult too. At absolute best, he showed this only for measles, and never connected the problem to the solution for mumps or rubella when he had to show all three. - That the good impacts of the model outweigh the harms
This is the point on which most of my analysis has been directed, and which I believe to be the most important. Pro had the burden to show this but his only substantive analysis was basically that it solves the problem. He never weighed that problem against the huge number of harms, just kept asserting that his model "trumps" mine. That's not enough. For example, I talked to you about third-party medical harms, a corrupt vaccine industry etc. Most of this has just been an assertion of denial from my opponent in response.
Return To Top | Posted:
 Judge: Blackflag
Judge: Blackflag
I think that nickname will stickPosted 2014-12-01 07:08:44
oooooooooooooooooooooooo snap
The Beast Slayer slayed the Beast once again!!!Posted 2014-12-01 06:42:55
I think everyone on this site needs a lesson in flow. Me foremost. Posted 2014-11-04 10:25:49
Lots of information is okay if it is well organized and relevant.
It is also important to maintain a flow of logic. Posted 2014-11-04 09:42:08
Yeah, thanks nzlockie. Got to admit spreading was definitely part of my strategy here.Posted 2014-11-04 09:38:59
nzlockie, I completely understand. This was an extensive debate that happened in two rounds, and I realize it got pretty messy, not to mention complex. I appreciate all of your feedback, as well as your thoughts on the debate and on our rounds, as it is still invaluable. If the worst that happens is that I lose this debate because we only have one voter, I have no complaints losing to Lars, especially not in a debate of this caliber.Posted 2014-11-04 08:42:30
Guys I'm sorry, I can't do it.
I've made four separate attempts to judge this debate and I just can't do it fairly. I'm going to abstain.
I have a little feedback for you though:
CON: It seemed that in this debate, right from the first round, your goal was to overwhelm me with examples. I don't know if this was your intention, but that's how it came across. You would often use four or five examples, where one or two would have sufficed. The positives of this was that I was left with the feeling that there was a mountain of evidence on your side. The negatives of this, was that I was left with a feeling that you were a little desperate and maybe even trying to distract me from something. Your impassioned speech against smoking for example had only the smallest relevance to the actual resolution.
Your graphs in the second round, especially the second one, needed labels. The explanation of them helped, but I shouldn't have to work so hard to figure out what the graph is showing. Graphs are supposed to make things easier, not harder.
The net result of all of this was that I constantly lost the thread of the debate. By the end of the CX I was scoring this a clear win for CON, but then PRO's second round argument came and he offered rebuttal for the hundred points CON had made. That's where I keep getting lost.
Final critique was that in your final round you submitted a LOT of new evidence which PRO would obviously have no chance to contest. I don't feel like this was fair, especially considering how close this had been.
On the positives, your case was very strong. If your intent was to swamp PRO's contentions, then you succeeded. That was definitely the impression I was left with.
I also appreciated your writing style which made long arguments easy to read.
PRO: Really the only critique I had for you was your second round argument. As mentioned above, this was where I got lost every time. I've thought about this a fair bit, and I THINK it comes down to your formatting. For every numbered point you put, I would go back and try and find that argument in CON's case. It would have helped if you'd have had a heading or something that got me there faster.
I typically HATE those rebuttals that are full of quotes, but in THIS case, that might have helped.
You DID give me the disclaimer at the beginning of that round, and I appreciated that.
On the positives, you deserve credit for pulling it back in the second half. Many times I felt like just writing this debate off as a win for CON based on the first half, but there was enough meat in your second round argument that I decided that a no-vote was the right way to go.
Sorry again for the no-vote guys!Posted 2014-11-04 08:01:10
Despite the fact that this is only a two round debate with CX, this must surely be a candidate for the longest debate...Posted 2014-10-29 14:20:51
This is going to be.... legendaryPosted 2014-10-08 10:51:18
Oh, it's on!Posted 2014-10-08 01:02:44
Alright, I would certainly be interested to see your case. I think there's a decent case to be had for Con, even there, just not a case I'd be all that excited to argue.Posted 2014-10-07 02:28:56
Actually I think I might have an ok case for con on reflection. Medicine topics aren't usually my thing but I don't have an MMR vaccination, so I feel like I ought to be able to answer for why that is. Time's not on my side though, so I won't take it unless it's still open at the very last moment.Posted 2014-10-06 17:36:25
;PPosted 2014-10-06 16:27:24
I hope this gets taken. You know you've got a seriously cool debate on when whiteflame starts pulling out acronyms before it even begins.Posted 2014-10-06 15:51:52
I was concerned about a valid line of argument, but I've had tougher resolutions
http://www.edeb8.com/debate/That+our+acquirement+of+knowledge+is+in+part+a+priori/Posted 2014-10-05 13:24:40
Learning by doing is very helpful. Tell you what - this topic is really easy for me to exploit by just running MMR, so I'll take a harder tack and argue for HPV vaccination being mandatory. Makes it a lot more even.Posted 2014-10-05 13:19:16
I really want to accept this debate, but I'm worried since you're also coaching me...
Posted 2014-10-05 11:53:05